This topic contains a solution. Click here to go to the answer
|
|
|

 Performing Transmission-Based Precaution: Isolation Techniques
Performing Transmission-Based Precaution: Isolation Techniques
 Performing a Gram Stain
Performing a Gram Stain
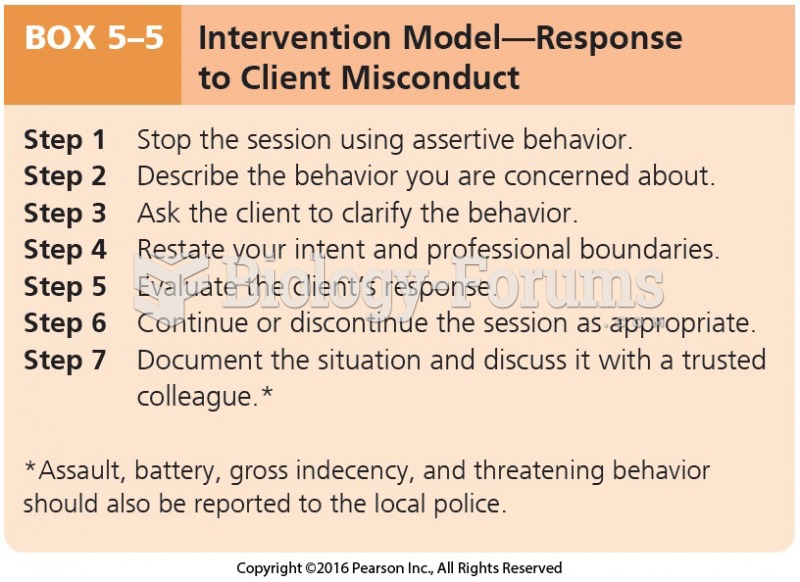 Intervention Model-Response to Client Misconduct
Intervention Model-Response to Client Misconduct
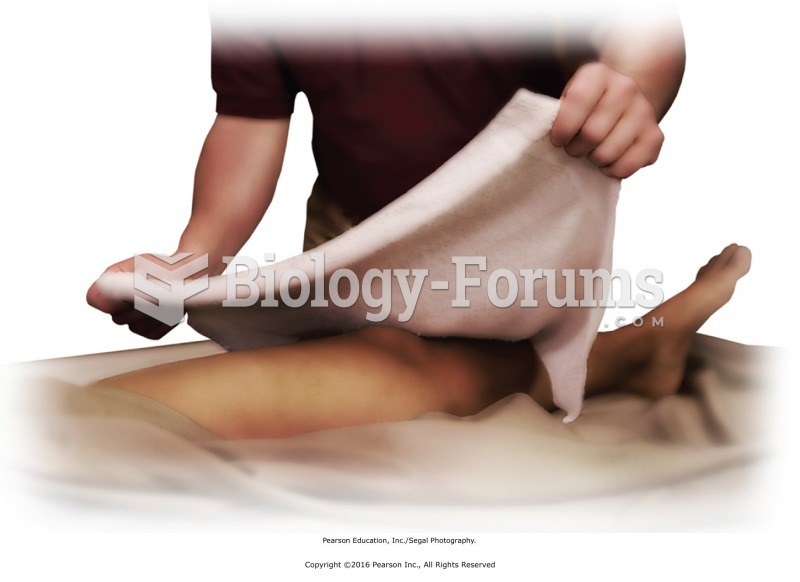 Place a towel or sheet over knee area. Use a thin barrier to protect skin from cold source.
Place a towel or sheet over knee area. Use a thin barrier to protect skin from cold source.
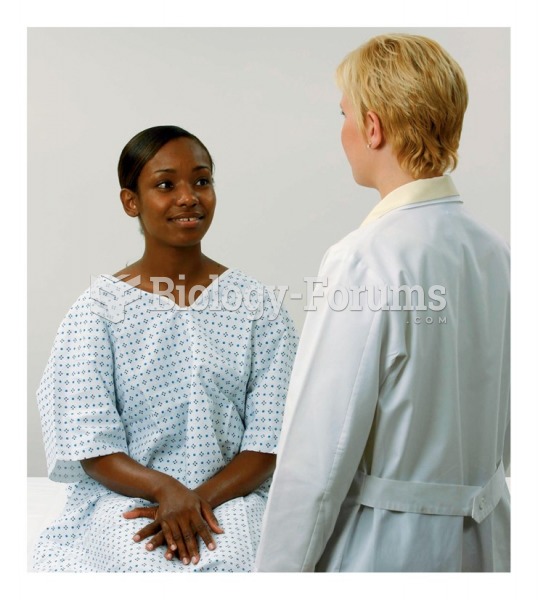 Positioning the client
Positioning the client
 Testing the client’s ability to feel vibrations, the toe
Testing the client’s ability to feel vibrations, the toe