This topic contains a solution. Click here to go to the answer
|
|
|

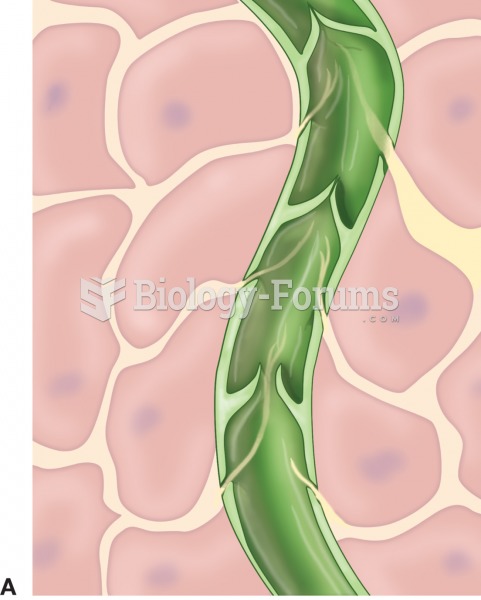 (A) Lymphatic vessel with valves within tissue cells; (B) photomicrograph of lymphatic vessel with v
(A) Lymphatic vessel with valves within tissue cells; (B) photomicrograph of lymphatic vessel with v
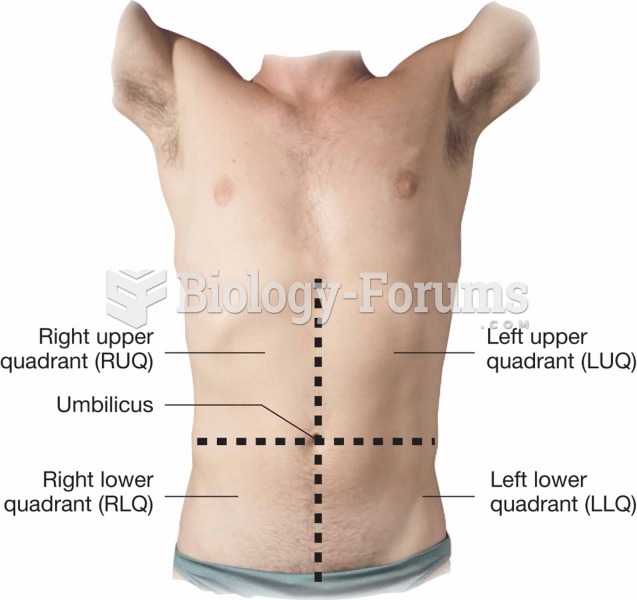 Quadrants of the abdominopelvic area
Quadrants of the abdominopelvic area
 Removing the sheet from underneath the client.
Removing the sheet from underneath the client.
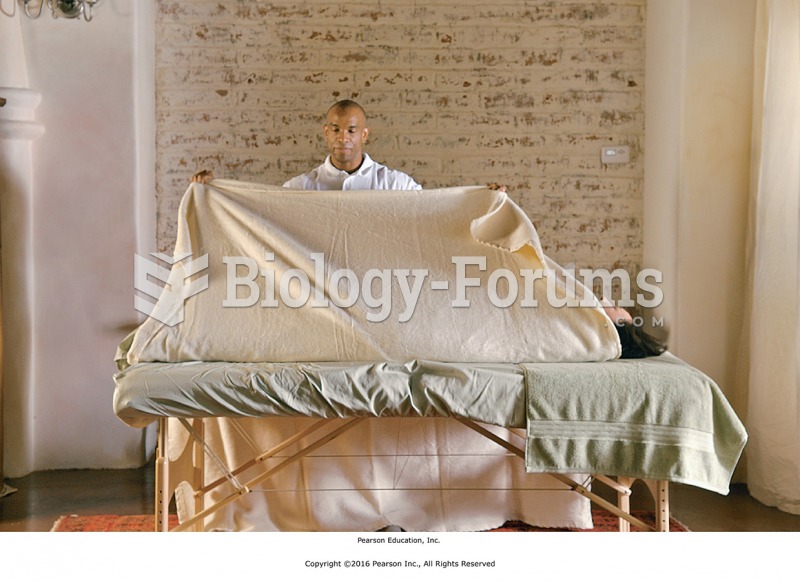 After the chemical exfoliation substance has been applied, wrap the two top sheets around the client ...
After the chemical exfoliation substance has been applied, wrap the two top sheets around the client ...
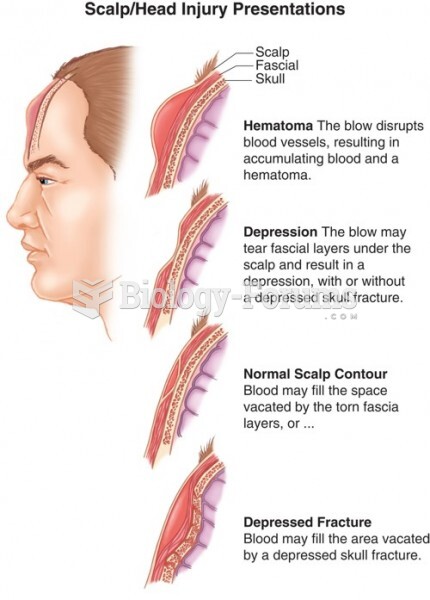 A Scalp/Head Injury Presentation
A Scalp/Head Injury Presentation
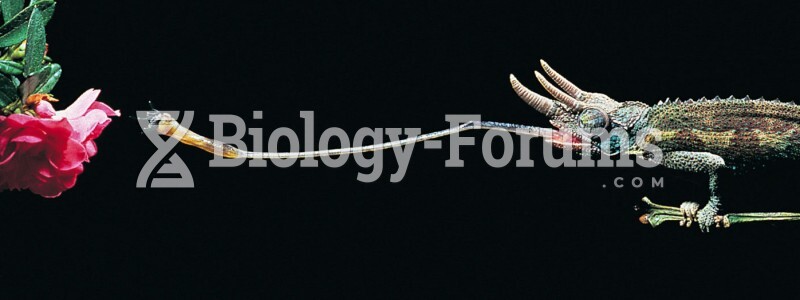 Example of a coordinated interaction between skeletal muscle tissue and nervous tissue
Example of a coordinated interaction between skeletal muscle tissue and nervous tissue