This topic contains a solution. Click here to go to the answer
|
|
|

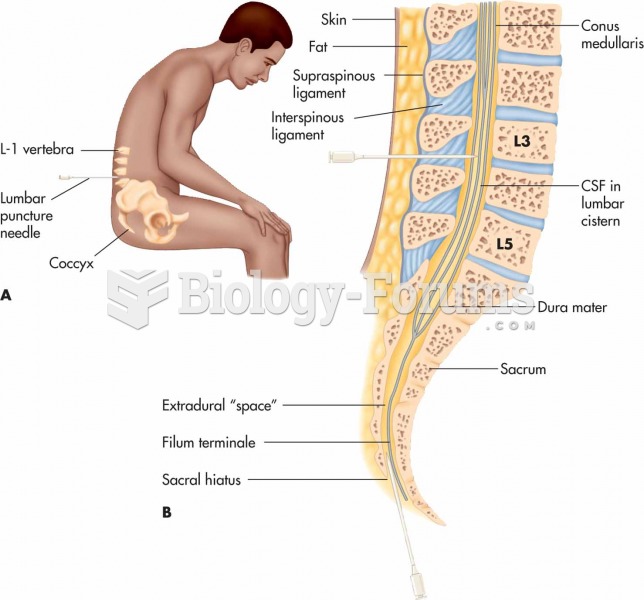 (A) Lumbar puncture, also known as spinal tap; (B) section of the vertebral column showing the spina
(A) Lumbar puncture, also known as spinal tap; (B) section of the vertebral column showing the spina
 The patient is undergoing an allergy skin test by receiving subdermal inoculations of allergens. Inf
The patient is undergoing an allergy skin test by receiving subdermal inoculations of allergens. Inf
 Skin-associated lymphoid tissue (SALT).
Skin-associated lymphoid tissue (SALT).
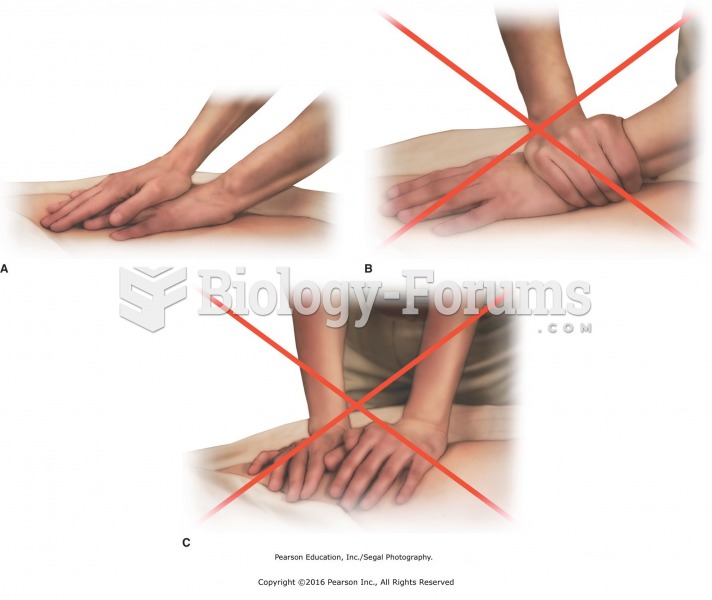 Correct wrist position while performing compression. A. Correct wrist position for compression ...
Correct wrist position while performing compression. A. Correct wrist position for compression ...
 Positioning the client
Positioning the client