Answer to Question 1
ANS: C
Documentation mistakes must be acknowledged. If an error is made in paper documentation, a line is drawn through the error and the word error is placed above or after the entry, along with the nurse's initials and followed by the correct entry. Notes should never be altered or obliterated. Documentation mistakes must be acknowledged.
Answer to Question 2
ANS: A
An admission summary includes the patient's history, a medication reconciliation, and an initial assessment that addresses the patient's problems, including identification of needs pertinent to discharge planning and formulation of a plan of care based on those needs. The discharge summary addresses the patient's hospital course and plans for follow-up, and it documents the patient's status at discharge. It includes information on medication and treatment, discharge placement, patient education, follow-up appointments, and referrals. Flow sheets and checklists may be used to document routine care and observations that are recorded on a regular basis, such as vital signs, medications, and intake and output measurements. Although computerization of records may mean that the Kardex system is no longer active, the term kardex continues to be used generically for certain patient information held at the nurses' station.

 The nurse conducts the health history as the first step in the nursing assessment
The nurse conducts the health history as the first step in the nursing assessment
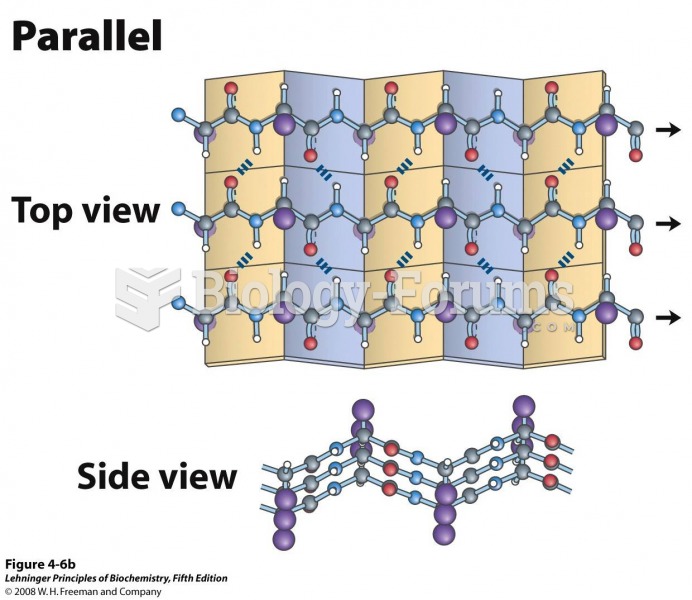 These top and side views reveal the R groups extending out from the β sheet and emphasize
These top and side views reveal the R groups extending out from the β sheet and emphasize
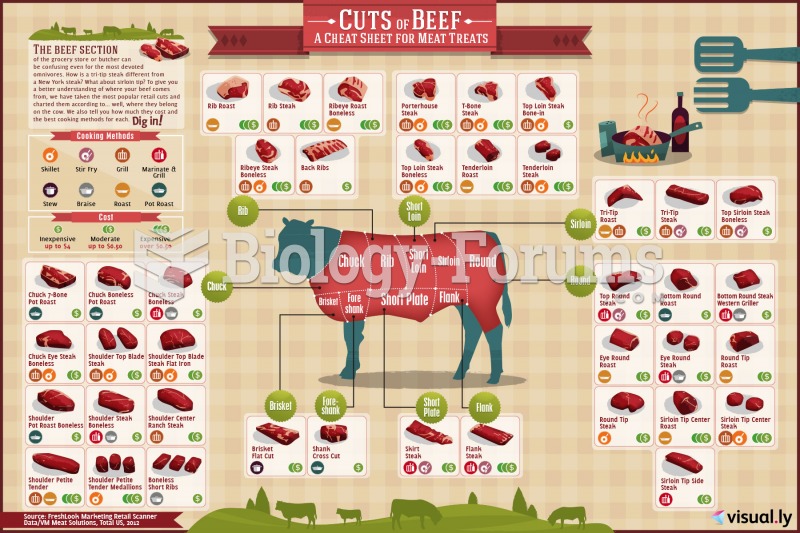 cheat sheet for cuts of beef.
cheat sheet for cuts of beef.
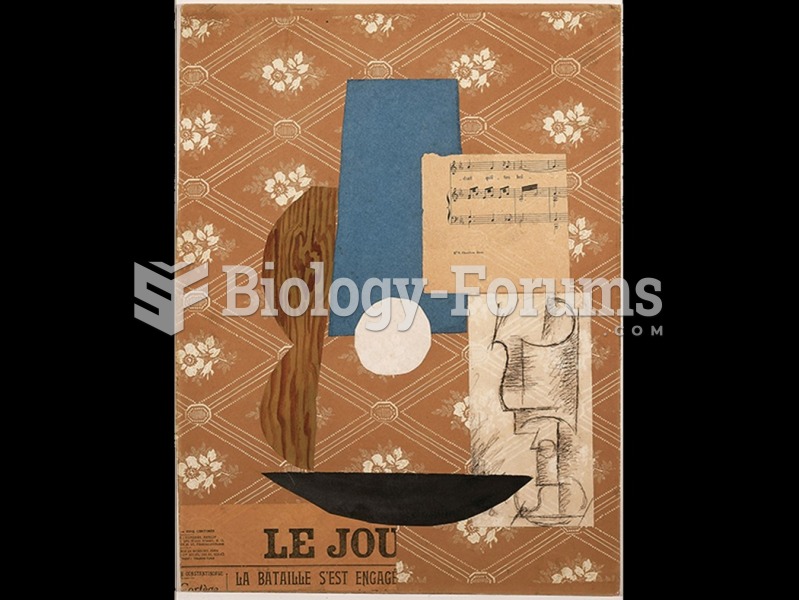 Pablo Picasso, Guitar, Sheet Music, and Wine Glass.
Pablo Picasso, Guitar, Sheet Music, and Wine Glass.
 Use caution if using a steel scraper to remove a gasket from aluminum parts. It is best to use a ...
Use caution if using a steel scraper to remove a gasket from aluminum parts. It is best to use a ...
 Place sheet or towel over area to be heated. Use sufficient heat barrier for the heat source used. ...
Place sheet or towel over area to be heated. Use sufficient heat barrier for the heat source used. ...