This topic contains a solution. Click here to go to the answer
|
|
|

 Vaccine Information Sheet (VIS) provided by the CDC for the varicella vaccination.
Vaccine Information Sheet (VIS) provided by the CDC for the varicella vaccination.
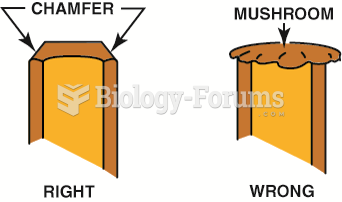 Use a grinder or a file to remove the mushroom material on the end of a punch or chisel.
Use a grinder or a file to remove the mushroom material on the end of a punch or chisel.
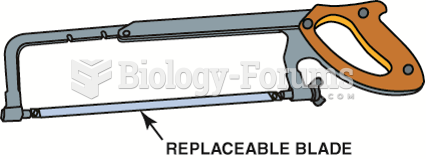 A typical hacksaw that is used to cut metal. If cutting sheet metal or thin objects, then use a ...
A typical hacksaw that is used to cut metal. If cutting sheet metal or thin objects, then use a ...
 Use caution if using a steel scraper to remove a gasket from aluminum parts. It is best to use a ...
Use caution if using a steel scraper to remove a gasket from aluminum parts. It is best to use a ...
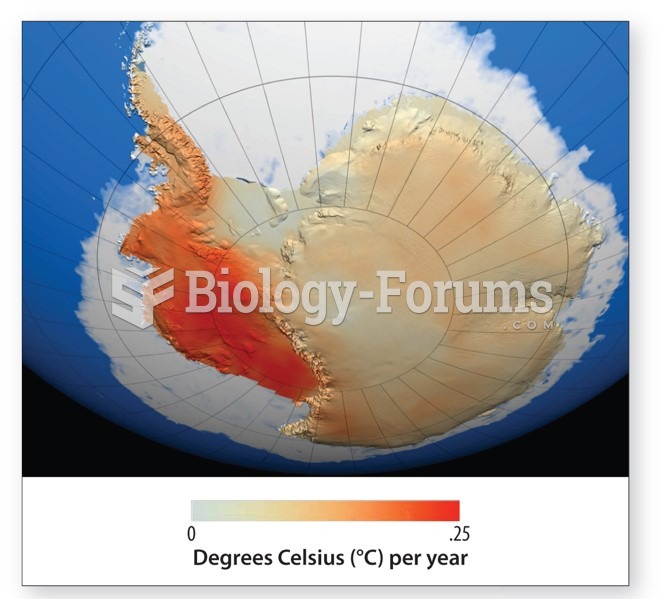 West and East Antarctic Ice Sheet
West and East Antarctic Ice Sheet
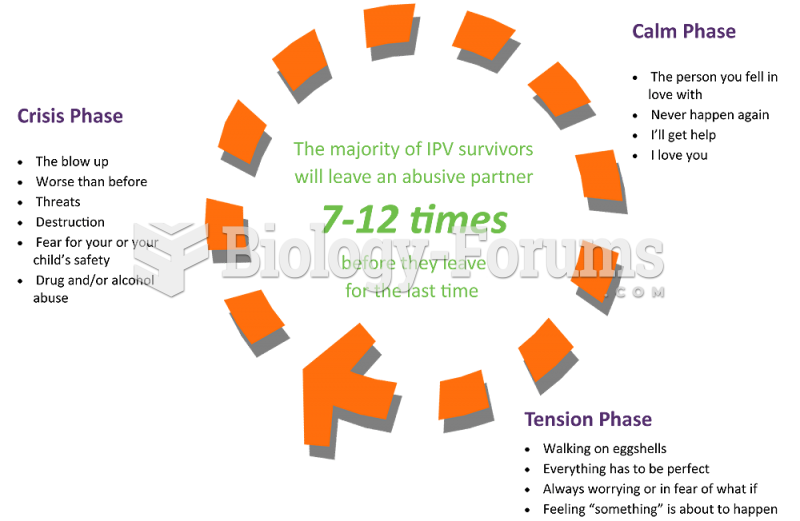 A patient is talking to the nurse about her husband’s abuse and attempt to strangle her. She ...
A patient is talking to the nurse about her husband’s abuse and attempt to strangle her. She ...