Answer to Question 1
D
Feedback
A Incorrect. Daily vitamin B12 intake is correct, but older adults require 20 to 35 g of fiber.
B Incorrect. 1600 calories per day is correct, but fluid intake (preferably water) should be 1500 ml, approximately six to eight 8-oz glasses.
C Incorrect. Vitamin B12 intake should be 2.4 mcg per day, and calories from fat should be 20 to 25.
D Correct. 1500 mg of calcium per day is recommended, and 600 to 800 units of vitamin D are needed to enable the body to utilize the calcium.
Answer to Question 2
A, B, E, F
An institution uses the same nursing documentation record because it helps provide continuity of care across various settings by providing organized, pertinent, and thorough health care data on a specific individual. Other units in the hospital and other health care settings have an easier time locating relevant data. Specific health care data are found in one location on a standardized nursing documentation record throughout an institution and provide the basis for standardized patient evaluation across settings. Standardized documents help describe patient acuity levels and thus provide a justification for staffing. Because the same parameters are, or should be, recorded across all units, the standardized documentation record allows for hospital-wide quality evaluations. Nurses must restrict access to a standardized documentation record or any other type of patient record such as laboratory reports, narrative or progress notes, and other documents. A standardized nursing documentation record can reduce a specific type of documentation error but is unlikely to affect the rate of medication errors.

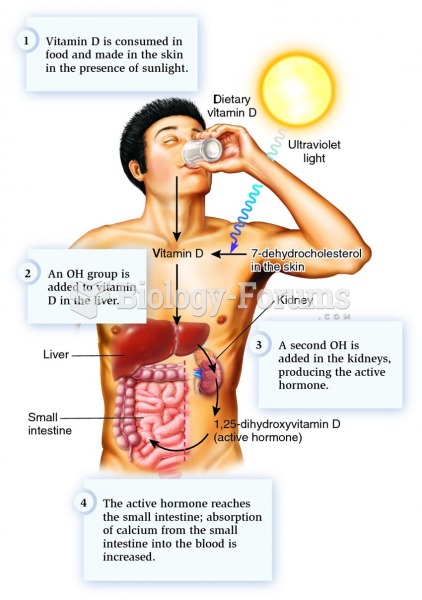 Synthesis of the active hormone formed from vitamin D or its precursor in skin.
Synthesis of the active hormone formed from vitamin D or its precursor in skin.
 A stallion with a proven competition record is one criterion for being a suitable sire.
A stallion with a proven competition record is one criterion for being a suitable sire.
 A combination wrench has an open end at one end and a box end at the other end.
A combination wrench has an open end at one end and a box end at the other end.
 Cross-fiber friction to the paraspinal muscles. Friction is created by moving the more superficial ...
Cross-fiber friction to the paraspinal muscles. Friction is created by moving the more superficial ...
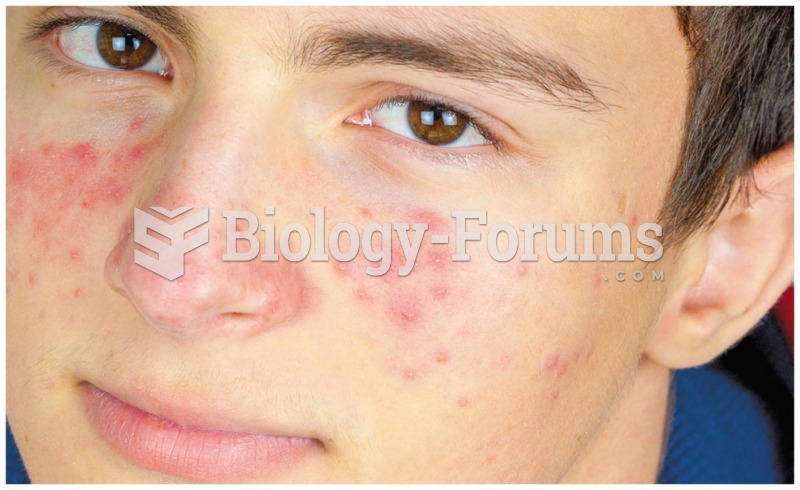 Vitamin A can aid in the treatment of acne
Vitamin A can aid in the treatment of acne
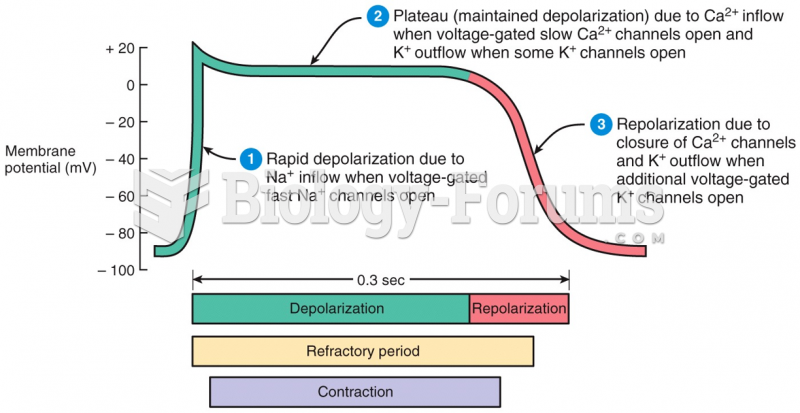 Action Potential in a Ventricular Fiber
Action Potential in a Ventricular Fiber