Code the following cases for inpatient facility purposes using ICD-9-CM and ICD-10-CM and PCS codes.
Calculate the MS-DRG.
Identify the Principal vs. Secondary diagnoses and procedures.
Use external cause codes when appropriate.
Do NOT code procedures that are captured by the facility chargemaster.
Secondary diagnoses and procedures do NOT need to be sequenced in any particular order. Enter "None" when no code is required.
If more than one occurrence of a procedure is required, report the code with "x 2""x 3" etc.
INPATIENT HOSPITAL
Health Record Face Sheet
Record Number: 82-50-77
Age: 81
Gender: Female
Length of Stay: 2 Days
Service Type: Inpatient
Discharge Status: To Long-Term Care
Diagnosis/Procedure: Severe Peripheral Venous Cellulitis Lower Extremities, Bilateral.
DISCHARGE SUMMARY
PATIENT: MYRA INPATIENT
RECORD NUMBER: 82-50-77
ADMITTED: 03-15-XX
DISCHARGED: 03-17-XX
PHYSICIAN: DR. ALEX, M.D.
DISCHARGE DIAGNOSIS: Severe peripheral venous cellulitis with 4+ edema lower extremities (bilateral).
HISTORY: This patient is an 81-year-old female admitted because of severe edema of her lower extremities and developing leg ulcers bilaterally.
LABORATORY DATA: SMAC showed glucose of 132, SGPT 29, albumin 3.2, cholesterol 258. The rest of the SMAC was normal. Urinalysis was physiologic. Hemoglobin 13.6, hematocrit 40.7, white count was 4,800 with a normal differential. Platelets were adequate. Red blood cell morphology was essentially normal.
HOSPITAL COURSE: The patient was admitted to the hospital to treat bilateral leg 4+ pitting edema and weeping infections of the sacrum and of both feet. Cultures of both the sacrum and feet were performed with cultures returning positive for staphylococcus aureus, methicillin susceptible, and Group A streptococcus. The patient was started on IV Tetracycline and Lasix. Edema of her feet cleared rapidly with simple elevation and two doses of Lasix. After discussion with the family, it was felt that long-term care placement was the most appropriate place to care for this patient.
DISCHARGE PLANS: Patient was transferred to the local long-term care facility with orders to remain mostly at bed rest with the legs elevated along with an order for heat lamp to the sacral area qid. Tetracycline treatment will continue as ordered for the next 5 days with review at that time. I suspected mild depression in the patient with orders to watch for increasing signs or symptoms with intervention as needed. The patient will be followed in the long-term care facility.
DR. ALEX, M.D.
Electronically authenticated by Dr. Alex, M.D., 03-18-xx 856
HISTORY AND PHYSICAL
PATIENT: MYRA INPATIENT
RECORD NUMBER: 82-50-77
ADMITTED: 03-15-XX
DISCHARGED: 03-17-XX
PHYSICIAN: DR. ALEX, M.D.
CHIEF COMPLAINT: Severe peripheral venous cellulitis with 4+ edema lower extremities (bilateral).
HISTORY OF PRESENT ILLNESS: This patient is an 81-year-old Caucasian female who lives alone and recently has lost her husband. The patient's daughter states that activities of daily living are accomplished only because of her help to the patient. The daughter checks on her mother three times a day to assure meals, baths, and general living activities. It is noted that the patient chooses to sleep in her chairs in the living room and not in her bed. The patient's legs reveal 4+ pitting edema and very swollen as her feet are down all day. She has weeping infections of both the sacrum and of both feet. The patient is alert and awake but does not seem interested in helping herself get better.
Home health has been seeing the patient on a bi-weekly basis but has stated that that the patient really cannot be managed at home any longer and needs to have other living arrangements for her own safety and health. She has been on no other medications.
ALLERGIES: She is allergic to Penicillin. Does not tolerate Codeine.
MEDICATIONS: Tetracycline. Hormone shot and Thyroxin.
FAMILY HISTORY: Family history of heart disease, diabetes, skin cancers.
PAST HISTORY: History of stroke eight months ago with resultant gait ataxia. She has had an appendectomy, total abdominal hysterectomy, a T&A, varicose vein operations and hemorrhoidectomy. She has had an adenomatous polyp with villous features removed from her colon in September. She has had skin cancers removed from her legs. Hypothyroidism.
REVIEW OF SYSTEMS: At this time, the patient has no complaints. She is a very reluctant patient and does not cooperate for examination. Patient denies any physical problems at this time.
PHYSICAL EXAMINATION:
GENERAL: Patient is awake, alert and noncooperative. There is weeping lesions of both feet and sacrum.
HEENT: Normocephalic without lesions. Fundi normal. She is wearing her dentures and does wear glasses. Hearing is good.
LUNGS: Clear to auscultation and percussion. No breast masses are noted.
HEART SOUNDS: Normal. Rhythm is regular.
ABDOMEN: Palpation of the abdomen reveals no masses. Bowel sounds are normal. There are no bruits.
PELVIC and RECTAL: Not attempted with this noncooperative patient. There is an area of skin breakdown over the sacrum and both feet are 4+ edematous with weeping from the dorsum of the feet.
ADMITTING DIAGNOSIS:
1. Severe edema with secondary infections of wounds of the sacrum and feet.
2. Cerebrovascular disease with previous stroke.
3. Hypothyroidism on replacement therapy.
PLAN: Admit for treatment of edema and weeping lesions of feet and sacrum.
DR. ALEX, M.D.
Electronically authenticated by Dr. Alex, M.D., 03-15- xx 8567
ICD-9-CM diagnosis code(s): PDx_____________________
SDx _____________________
ICD-9-CM procedure code(s): PPx_____________________
SPx_____________________
ICD-10-CM diagnosis code(s): PDx_____________________
SDx _____________________
ICD-10-PCS procedure code(s): PPx_____________________
SPx_____________________
MS-DRG: _____________________

 Booker T. Washington in his office at Tuskegee Institute, 1900. Washington chose a policy of accommo
Booker T. Washington in his office at Tuskegee Institute, 1900. Washington chose a policy of accommo
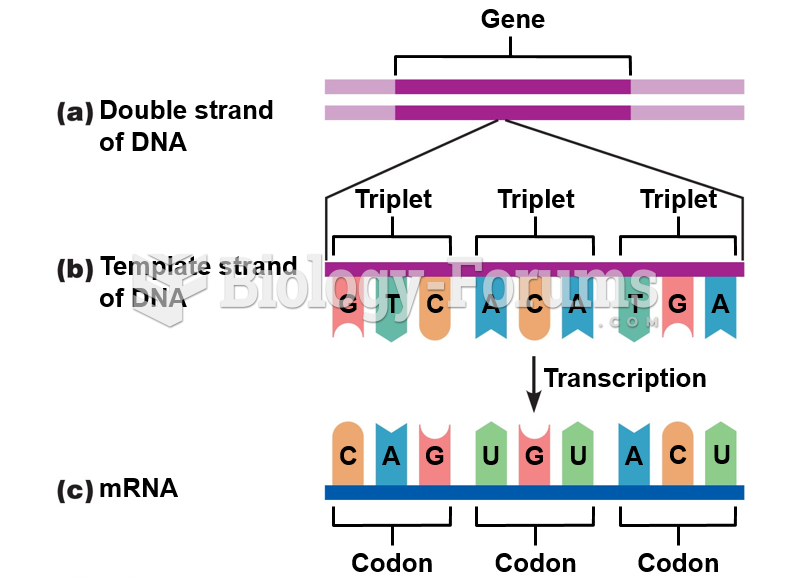 The genetic code.
The genetic code.
 Medical assistants who perform billing must know and use the proper codes to ensure third-party ...
Medical assistants who perform billing must know and use the proper codes to ensure third-party ...
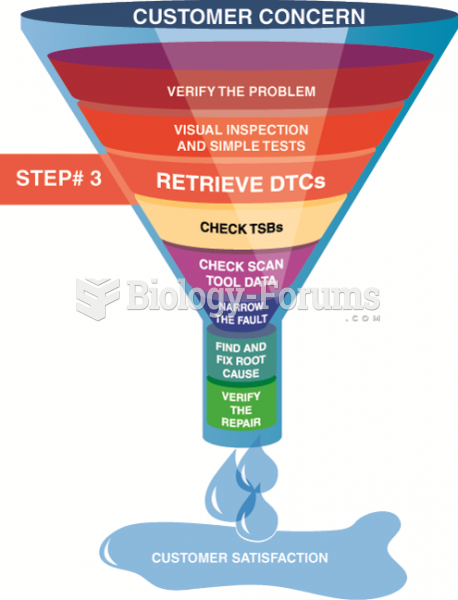 Step 3 in the diagnostic process is to retrieve any stored diagnostic trouble codes.
Step 3 in the diagnostic process is to retrieve any stored diagnostic trouble codes.
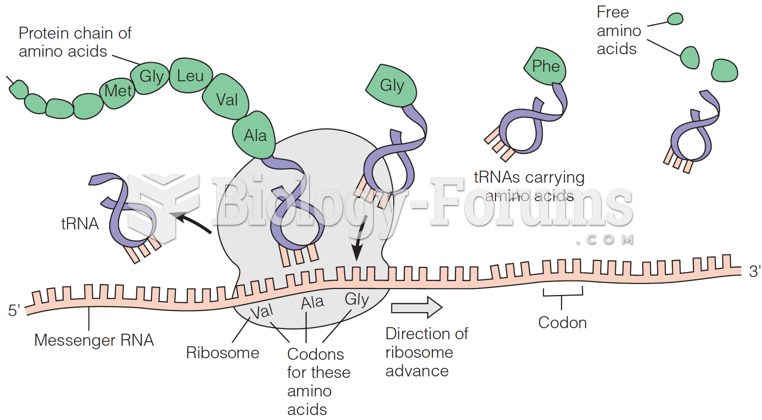 genetic code: The basic principle of translation
genetic code: The basic principle of translation
 Strategic Management: Concepts and Cases
Strategic Management: Concepts and Cases