Code the following cases for inpatient facility purposes using ICD-9-CM and ICD-10-CM and PCS codes.
Calculate the MS-DRG .
Identify the Principal vs. Secondary diagnoses and procedures.
Use external cause codes when appropriate.
Do NOT code procedures that are captured by the facility chargemaster.
Secondary diagnoses and procedures do NOT need to be sequenced in any particular order.
Enter "None" when no code is required.
If more than one occurrence of a procedure is required, report the code with "x 2""x 3" etc.
INPATIENT HOSPITAL
Health Record Face Sheet
Record Number: 79-50-77
Age: 36
Gender: Female
Length of Stay: 5 Days
Service Type: Inpatient
Discharge Status: To Home
Diagnosis/Procedure: Insulin reaction
Renal failure
Diabetes Mellitus, Type II, long term insulin dependence
Permanent catheter right internal jugular
Removal peritoneal dialysis catheter
DISCHARGE SUMMARY
PATIENT: RAINEY INPATIENT
RECORD NUMBER: 79-50-77
ADMITTED: 12-19-XX
DISCHARGED: 12-24-XX
PHYSICIAN: DR. ALEX, M.D.
DISCHARGE DIAGNOSES:
1. Insulin reaction.
2. Renal failure.
3. Diabetes mellitus, Type II.
OPERATIONS/ PROCEDURES:
1. Permanent catheter right internal jugular.
2. Removal of peritoneal dialysis catheter.
DISCHARGE MEDICATIONS:
1. Ceftin 250 mg bid.
2. Reglan.
3. Prilosec.
4. Iron.
5. Procardia.
HISTORY: This patient is a 36-year-old woman who was admitted because of insulin reaction, nausea, and vomiting. She has renal failure. The plan was to admit her for placement of a permanent access catheter for dialysis and she had an insulin reaction with a blood sugar of 17 Dextrostrip prior to the admission. She was given Glucagon in the unit. An IV was started in the emergency room. She was given D5 and water. She had been experiencing nausea and had not eaten as well as probably was necessary as an outpatient.
LABORATORY DATA: EKG showed T-wave inversion inferiorly and ST segment depression, stable and on specific. Urine culture and blood culture at the time of this dictation reveals no growth. SMAC showed a creatinine of 7.0, BUN 34, glucose 208, uric acid 5.9, alk. phos. 283, SGOT 238, LDH 294, total protein 4.7, albumin 1.4 grams, sodium 130, potassium 3.5, chloride 95 millimoles per liter, cholesterol 111, the rest of the SMAC was normal. Hemoglobin on admission had been 10.8, hematocrit 32.5, white count 4.1K with a normal differential. Platelets were adequate. The hematocrit was 17.8 the day before discharge. She was given one unit of packed red blood cells. Chest x-ray showed significant improvement on 12-21 of the pleural effusion she had had on previous films.
HOSPITAL COURSE: The patient was admitted to the hospital with an insulin reaction and given intravenous glucose as above after she had had an insulin reaction in the field and glucagon had been given. She received Prilosec and Reglan intravenously initially and then the Reglan was changed to oral. I gave it 2 hours before the meal. This seemed to enable her to eat and retain food. She had a slight fever. Cultures of the urine and blood were obtained but no growth was present so far. She had been on Cipro as an outpatient. I did not think any catheters were infected nor was there any evidence of peritonitis from the peritoneal dialysis. The peritoneal dialysis catheter had been removed during this hospital stay and another catheter placed in the right upper chest. I treated her empirically with Fortaz after obtaining cultures. The morning of Dec 24th, she was very anxious to go home for Christmas. I told her that I recommended she stay in the hospital to take the intravenous antibiotics and continue to monitor things as we had had such a difficult time controlling the blood sugar ranging from nearly 900 one day to below 50 the next. She, however, was well oriented, understood the situation, and definitely wanted to leave the hospital for Christmas with her family.
DISPOSTION: She was discharged on 12/24. She would take her usual medications at home except would d/c the Cipro and take Ceftin 250 mg bid. She would continue Reglan, Prilosec, Iron and Procardia. Dialysis would be again on Thursday and then again on Saturday. Follow up in about one week in the office.
DR. ALEX, M.D.
Electronically authenticated by Dr. Alex, M.D., 12-26-xx 5568
HISTORY AND PHYSICAL
PATIENT: RAINEY INPATIENT
RECORD NUMBER: 79-50-77
ADMITTED: 12-19-XX
DISCHARGED: 12-24-XX
PHYSICIAN: DR. ALEX, M.D.
CHIEF COMPLAINT: Severe renal failure secondary to very brittle diabetes mellitus, Type II, with long-term treatment with insulin.
HISTORY OF PRESENT ILLNESS: Severe renal failure secondary to very Type II diabetes mellitus, long-term treatment with insulin. This patient with renal failure was previously on peritoneal dialysis. She is not tolerating peritoneal dialysis due to very low total protein and albumin. This patient needs a more permanent hemodialysis access. We will place a temporary subclavian or temporary jugular catheter. The patient is being admitted to the hospital at this time for placement of dialysis catheter via one of the internal jugular sites.
DRUG ALLERGIES: None known.
PERSONAL MEDICAL HISTORY: Otherwise unremarkable. Most recently, she had a severe episode of hypoglycemia. The patient subsequently went home and was admitted to the hospital the morning surgery was to be accomplished having been found by her mother cold and with a very low blood sugar. She was brought to the emergency room and taken straight to the floor where she responded.
FAMILY HISTORY: Paternal grandmother with diabetes mellitus.
REVIEW OF SYSTEMS: Otherwise unremarkable.
PHYSICAL EXAMINATION:
VITAL SIGNS: Temperature is 87.5. Blood pressure of 153/86, pulse of 85, respirations 16.
GENERAL: The patient felt cold.
HEENT/NECK: Otherwise unremarkable.
LUNGS: Clear to auscultation and percussion.
CARDIOVASCULAR: Regular sinus rhythm.
ABDOMEN: Benign.
EXTREMITIES: Unremarkable.
IMPRESSION: Severe renal failure secondary to very brittle diabetes mellitus, Type II, long-term dependence on insulin.
RECOMMENDATIONS: Placement of perm-cath through one of the internal jugular sites.
DR. ALEX, M.D.
Electronically authenticated by Dr. Alex, M.D., 12-26-xx 5568
OPERATIVE REPORT
PATIENT: RAINEY INPATIENT
RECORD NUMBER: 79-50-77
SURGERY DATE: 12-19-XX
DISCHARGED: 12-24-XX
PHYSICIAN: DR. ALEX, M.D.
PREOPERATIVE DIAGNOSIS: Chronic renal failure in a very brittle diabetic, unable to tolerate peritoneal dialysis because of loss of protein and albumin.
POSTOPERATIVE DIAGNOSIS: Chronic renal failure in a very brittle diabetic, unable to tolerate peritoneal dialysis because of loss of protein and albumin.
OPERATIVE PROCEDURE: Cut down placement of permanent catheter right internal jugular and removal of peritoneal dialysis catheter.
ANESTHESIA: General endotracheal.
DESCRIPTION: The patient was taken to the operating room having been put to sleep, endotracheal tube in place. She had Betadine prep of the entire neck, jaw, and upper thorax down to the nipples. She also had prep of the left lower quadrant around the permanent catheter. She had a sterile drape in both areas. Attention was turned towards placing the permanent catheter. Initially, a transverse incision was made in the skin line, distal third of the neck on the right, transverse fashion and carried down through platysma muscle. Hemostasis was obtained with a Bovie. Flaps were developed inferiorly and superiorly, sufficient to allow muscle-splitting incision through anterior body sternocleidomastoid muscle. The dissection was carried straight down. Deep fascia of the neck was encountered and there was marked scarring in this location. The patient had a previous temporary dialysis catheter long term on this side. The carotid artery was palpated and adjacent to the artery just laterally. The lateral border of the scarred, whitish colored wall of the internal jugular vein was identified. With gradual dissection over the top of this, we were able to isolate the jugular vein from the carotid artery, taking care not to injure the vagus nerve. The vein was dissected free from a distance of approximately 2 cm, vascular tape was passed without difficulty. Dissection was prolonged because of the dense tissue in this region. We were able to get around this without entering the vessel. A #4-0 Prolene vascular purse string was then placed in Trendelenburg position. Ends were placed inferiorly on the purse string so that it could be tied directly down on the vein. The catheter was then inserted after what was felt to be the appropriate length was selected. Incision was then made so a #36 French catheter could be inserted through skin tunnel located below the clavicle on the right side and brought through a portion of the muscle to allow for adequate bend without kinking. Once this was accomplished, the internal jugular was lifted anteriorly with the Bakke pickups and a #15 blade was used to make an opening in the vein.
The vein, as indicated, was scarred and sclerosed, however, an opening was made sufficient to allow placement of the catheter without difficulty. In the process, approximately 25 cc of blood was lost. The purse string was then tied down. There was a small leak on the superior aspect and stick tie of #4-0 Vascular Prolene was then sewed to secure this. X-ray was obtained and catheter was seen in the part of the superior vena cava, and it was pulled out approximately 2 cm so that the pledget regressed still just inside the skin. This was accomplished and wound was irrigated. A #2-0 Vicryl was used to approximate the deep fascial layer of the neck and platysma muscles also approximated with #2-0 Vicryl. A #4-0 Vicryl was used subcuticular and Steri-Strips were used on the skin. The wound was dressed and tegaderm was placed over the catheter where it came out of the skin. Attention was then turned towards the peritoneal dialysis catheter. Dressings were removed off of this location and cut so we could get down to where the catheter had been inserted just above the iliac crest on the left. The incision for insertion was well above where the catheter went. It was a good 6 cm above where the catheter failed to go. A ¼ -inch incision was made directly over where we thought the catheter was inserted on the lateral border of the rectus muscle. Hemostasis was obtained with a Bovie after incision was made in the skin. With blunt dissection, we were able to go down and identify the catheter, go through the abdominal wall musculature. This was identified just lateral to the edge of the rectus. The catheter was then grasped. It was cut in this location and the pledget was placed near the skin, was removed after making a 1½ cm incision along the tract of the catheter down to its junction with the peritoneum. This was identified. The catheter was pulled back after it was removed and there adherent omentum on the catheter in this location. This was transected after being clamped with a small clamp, the end of the omentum tied off with #2-0 silk, and the omentum was tucked back into the abdominal cavity. The edges of the peritoneum and fascia, which were hypertrophied, were grasped with clamps and three #3-0 stick ties of #0 Vicryl were used to close this opening in the peritoneum.
The wound was irrigated and the fascial layer anteriorly was then used to approximate the subcuticular layer and #4-0 Prolene used to run and close skin. Accu-Chek prior to coming back to the ICU approximately 30 minutes before case was over was 230. The patient had no complications during surgery. She was sent to the recovery room with stable vital signs.
DR. ALEX, M.D.
Electronically authenticated by Dr. Alex, M.D., 12-26-xx 5568
ICD-9-CM diagnosis code(s): PDx_____________________
SDx _____________________
ICD-9-CM procedure code(s): PPx_____________________
SPx_____________________
ICD-10-CM diagnosis code(s): PDx_____________________
SDx _____________________
ICD-10-PCS procedure code(s): PPx_____________________
SPx_____________________
MS-DRG: _____________________

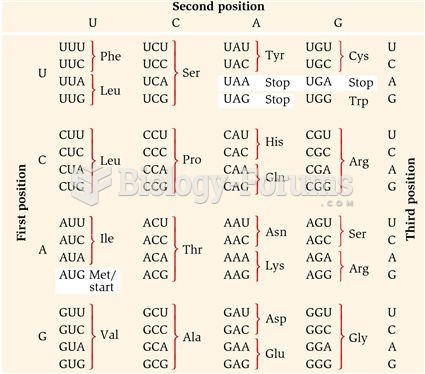 The Genetic Code
The Genetic Code
 The vehicle’s fuel pump is disabled by removing its relay or fuse. In some cases, it may be ...
The vehicle’s fuel pump is disabled by removing its relay or fuse. In some cases, it may be ...
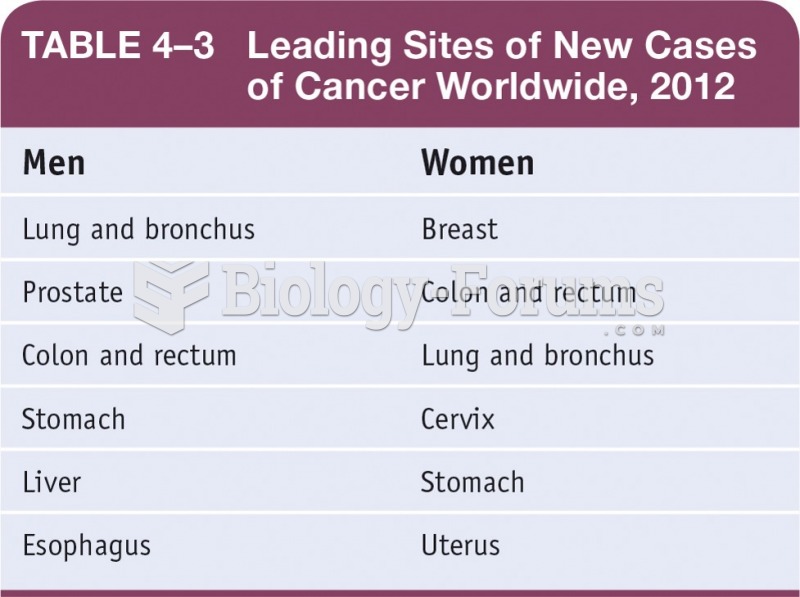 Leading Sites of New Cases of Cancer Worldwide, 2012
Leading Sites of New Cases of Cancer Worldwide, 2012
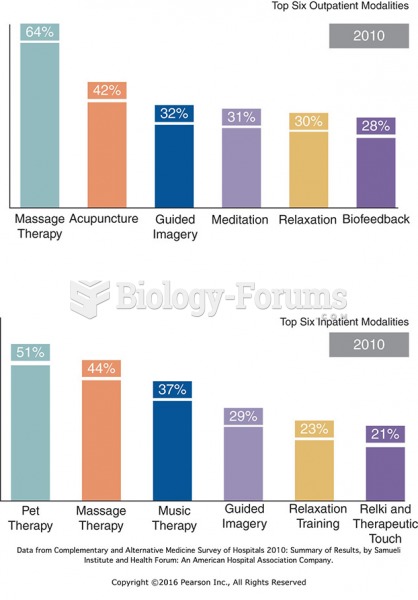 Top Six Hospital Outpatient and Inpatient CAM Therapies.
Top Six Hospital Outpatient and Inpatient CAM Therapies.
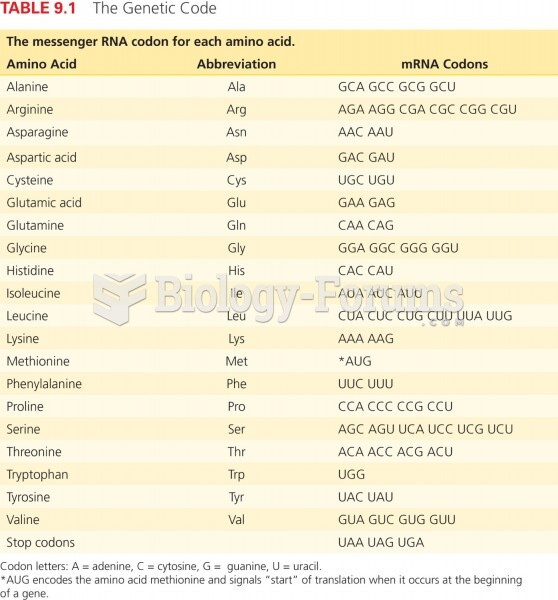 The Genetic Code
The Genetic Code
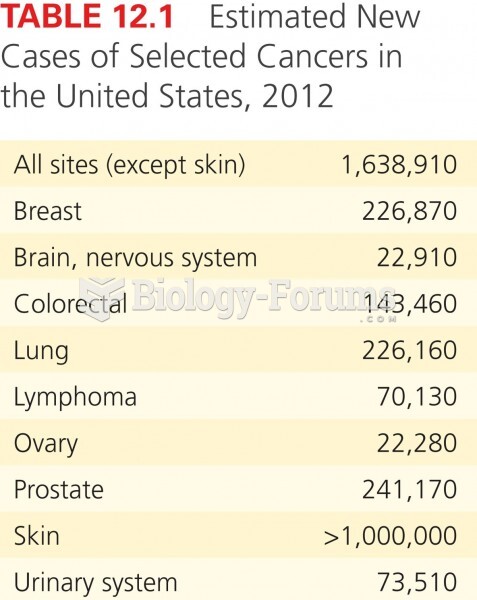 Estimated New Cases of Selected Cancers in the USA, 2012
Estimated New Cases of Selected Cancers in the USA, 2012