Answer to Question 1
The reason for the high incidence of hypertension among African Americans is not entirely clear. Salt sensitivity, or the increase of blood pressure in response to a high-sodium diet, has been speculated. This condition is thought to involve an impaired renal sodium transport mechanism. Increased vasomotor tone and abnormal endothelium-dependent vasodilation are other possibilities for the prevalence of hypertension among African Americans.
Barriers to care are noteworthy in this population. There are frequently financial considerations, difficulties in accessing health care, or long wait times for treatment. Furthermore, health education materials may not be culturally sensitive and fail to address the high rate of salt sensitivity, smoking, and obesity among African Americans.
An elevated systolic pressure, even in the absence of diastolic hypertension, carries with it a high risk for cardiovascular disease. Increased systole is associated with left ventricular hypertrophy, increased myocardial demand for oxygen, and subsequent heart failure. An absolute or relative decrease in diastolic pressure limits coronary perfusion. Finally, a widened pulse pressure damages arterial tissues and predisposes an individual to atherosclerosis and aneurysm formation.
Diuretics reduce blood pressure by increasing renal secretion of sodium and water. They reduce cardiac output and with prolonged use, decrease peripheral vascular resistance. ACE inhibitors limit the activity of ACE in converting angiotensin I to angiotensin II. As a result, less circulating angiotensin II is available to trigger aldosterone secretion and vasoconstriction. ACE inhibitors also inhibit bradykinin degradation and stimulate the production of prostaglandins that have a vasodilating effect.
Answer to Question 2
An elevated ST segment is indicative of acute, transmural ischemia. The result is a decreased resting membrane potential and shortened action potential in damaged myocardial fibers. The current of injury is what appears on the electrocardiogram. Variables affecting the ECG produced include the duration of the ischemic event, the extent of myocardial damage, and the location of the injury in the cardiac tissue.
Myocardial ischemia triggers anaerobic metabolism and subsequent inability for the heart to produce enough energy to function adequately. Fibrinolytic therapy dissolves clot formations so that reperfusion can occur and prevent, or limit, necrosis and microvascular damage. Nitroglycerin mimics endogenous nitric oxide from endothelial tissue and acts as a vasodilator to increase blood flow to cardiac tissue. Vasodilation reduces preload and afterload, therefore reducing demands on the heart. Because nitroglycerin relieves the pain associated with MI, it may assist in the reduction of the sympathetic response. This also contributes to decrease metabolic demand on the heart. The administration of oxygen increases hemoglobin saturation levels to ensure well-oxygenated blood is present in the coronary circulation.
Myocardial damage typically involves a necrotic zone, an area of injury, and an ischemic region. The inner necrotic zone is incapable of recovery or repair. The inflammatory response involves the migration of macrophages to this area to remove the necrotic tissue and cellular debris. Following this process is the lay down of granulation tissue and subsequent deposition of fibrin. Scar tissue finally replaces the area of ischemic insult and has the effect of decreasing extensibility and contractility of the cardiac wall. The initiation and conduction of action potentials are also compromised in the noncontractile area.

 African bush (savanna) elephant in Etosha National Park, Namibia.
African bush (savanna) elephant in Etosha National Park, Namibia.
 Skin of an African (left) and Asian (right) elephant.
Skin of an African (left) and Asian (right) elephant.
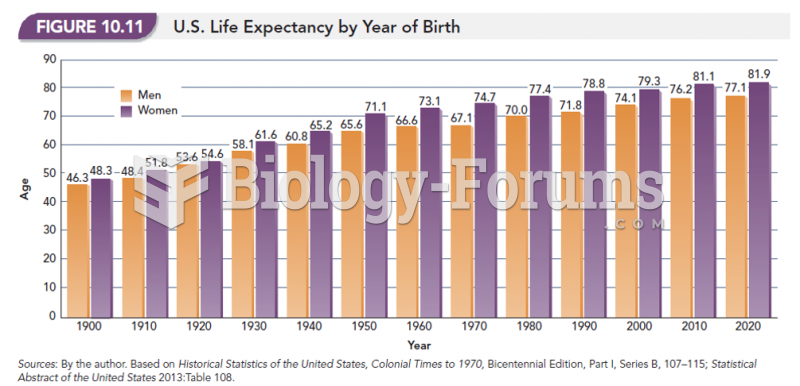 U.S. Life Expectancy by Year of Birth
U.S. Life Expectancy by Year of Birth
 Distribution of Thunderstorms: Approximately 14.5 million thunderstorms occur each year across the ...
Distribution of Thunderstorms: Approximately 14.5 million thunderstorms occur each year across the ...
 A non-interest-bearing five-year note for $54600.00 issued May 1, 2015, is discounted April 1, ...
A non-interest-bearing five-year note for $54600.00 issued May 1, 2015, is discounted April 1, ...