Answer to Question 1
ANS: A
Gestational diabetes mellitus (GDM) involves glucose intolerance that develops or is first discovered during pregnancy and hence may include women who have undiagnosed pre-gestational diabetes. A pregnant woman may be asymptomatic throughout the entire pregnancy or may report classic episodes of polyuria, polyphagia, or polydipsia. She may experience episodes of UTIs or vaginitis; therefore, recurrent infections should signal an earlier screening for diabetes or at least a random glucose level. Obstetric history should be investigated for unexplained stillbirths, spontaneous abortions, unexplained preterm birth, low birth weight (with undiagnosed preexisting diabetes), newborn weighing 4,000 g or more, or a previous incident of major congenital abnormality. Family history should be explored for diabetes, including GDM.
Maternal age and weight should be noted because major risk factors include an age over 35 years or a pre-pregnancy weight of more than 200 pounds. Excessive weight gain during pregnancy or a fundal height greater than expected is also worrisome. The blood pressure should be noted because women with diabetes are predisposed to hypertensive disorders, including pre-eclampsia. A retinal examination should be completed to assess for retinopathy. A urine dipstick should be evaluated for glycosuria and proteinuria.
Differential Diagnoses
GDM, undiagnosed type 1 DM or type 2 DM, hyperglycemia, macrosomia, recurrent UTI or vaginitis (not related to DM).
Universal screening continues to be widely practiced within the United States between 24 and 28 weeks of gestation with a 50-g, 1-hour Glucola test using a venous blood sample. There are two thresholds for an abnormal test: (1) A fasting plasma glucose cutoff of 85 mg/dL will identify 87 of the women who will have a subsequent positive 100-g, 3-hour oral glucose challenge test (OGCT) and (2) a cutoff of 140 mg/dL will detect 80 of women who will have a subsequent abnormal OGCT but will decrease the number of false positives (Beukema, Raiche, & Turok, 2008; USPSTF, 2013). Although both tests are similar in ruling out GDM, the OGCT is superior in identifying women with GDM. Glycated hemoglobin level (HbA1c) changes lag behind changes in serum glucose by months. It is therefore not a good screen for GDM since glucose elevations do not often start to occur until after 20 weeks' gestation (USPSTF, 2013). A fasting blood sugar (FBS) should be checked, and if it is elevated (above 85 to 95 mg/dL), the woman should be considered as having GDM. If the FBS is under 85 mg/dL, a 3-hour OGCT should still be done.
The 3-hour OGCT is usually administered after an overnight fast for at least 8, but not more than 14, hours. An FBS is obtained, and then a 100-g glucose load is given. Venous blood sugar samples are then obtained at 1, 2, and 3 hours after the glucose load. Either an elevated FBS or two elevated values on the 3-hour OGCT is diagnostic of GDM. If only one value on the OGCT is elevated, the test should be repeated between 32 and 34 weeks of gestation.
Answer to Question 2
ANS: B
Determination of the woman's nonpregnant blood pressure is important in the evaluation of blood pressure during pregnancy. Gestational HTN is defined as a systolic blood pressure of 140 mm Hg or higher or a diastolic blood pressure of 90 mmHg or higher that occurs after 20 weeks of gestation in a woman with previously normal blood pressure (ACOG, 2002). The past 3015 rule, which followed elevations of systolic blood pressure increases by more than 30 mm Hg or diastolic increases of more than 15 mm Hg over baseline, has not been proven to be a good prognostic indicator. However, pre-eclampsia may still occur even if the blood pressure is still within the accepted normal range, and women who demonstrate the 3015 rule still warrant close observation. A certain degree of caution should also be displayed for women with a blood pressure of 120/75 mm Hg or higher in midpregnancy or 130/85 mm Hg in later pregnancy (Lindheimer & Akbari, 2000).
Evaluation should include the presence of edema, blood pressure measurement, urine dip or 24-hour urine for proteinuria, CBC or platelet count, liver enzymes, reflex testing, retinal changes, hepatomegaly, or right upper quadrant tenderness.

 A visually impaired patient is assisted by a service dog.
A visually impaired patient is assisted by a service dog.
 A patient with exophthalmos.
A patient with exophthalmos.
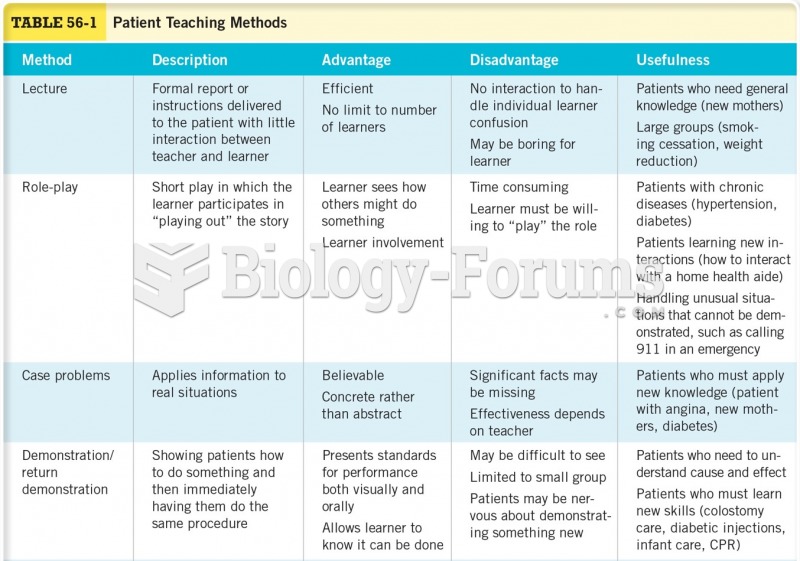 Patient Teaching Methods
Patient Teaching Methods
 Patient with DiGeorge syndrome. Note low set ears and wide set downward slanting eyes; often these ...
Patient with DiGeorge syndrome. Note low set ears and wide set downward slanting eyes; often these ...
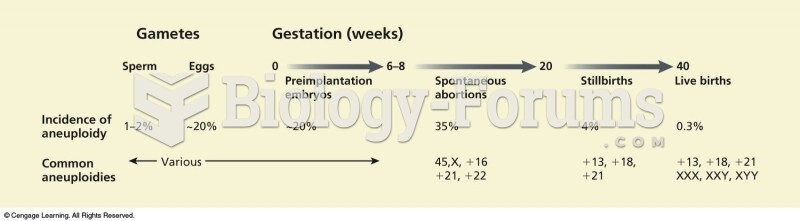 The frequency of aneuploidy changes dramatically over developmental time. Between 6 to 8 weeks and 2
The frequency of aneuploidy changes dramatically over developmental time. Between 6 to 8 weeks and 2
 Earth 150 Million Years Ago
Earth 150 Million Years Ago