Answer to Question 1
D
Most patients with Guillain-Barr syndrome (GBS) do not require admission to the critical care unit. However, the prototype of GBS, known as acute inflammatory demyelinating polyradiculoneuropa thy (AIDP), involves a rapidly progressive, ascending peripheral nerve dysfunction, which leads to paralysis that may produce respiratory failure. Because of the need for ventilatory support, AIDP is one of the few peripheral neurologic diseases that necessitates care in a critical care environment
Answer to Question 2
B
If the monitored heart has a normal electrical axis, lead II displays a waveform that is predominantly upright, with a positive P wave and positive QRS waveform. P waves are usually easy to identify in lead II, and it is recommended for monitoring of atrial dysrhythmias. However, it is difficult to identify right bundle branch block (RBBB) and left bundle branch block (LBBB). The selection of an electrocardiographi c monitoring lead is not a decision to be made casually or according to habit. The monitoring lead should be chosen with consideration of the patient's clinical condition and recent clinical history. Lead V1 is the optimal lead to select if the critical care nurse needs to analyze ventricular ectopy. V1 provides information to facilitate differentiation between RBBB versus LBBB pattern or distinguish between ventricular tachycardia and supraventricular tachycardia with aberrant conduction; determine whether premature ventricular contractions originate in the right or left ventricle, and clarify when ST segment changes are caused by the RBBB and when they are the result of ischemia. Lead V1 is excellent for this purpose. MCL1 is an uncommon lead choice today. It is used only if monitoring with a three-lead system such as on a transport monitor.

 Stevens-Johnson Syndrome
Stevens-Johnson Syndrome
 Polycystic ovary syndrome.
Polycystic ovary syndrome.
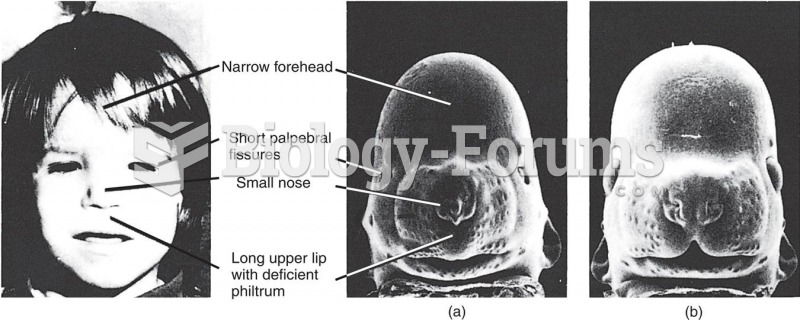 Facial Malformations in Fetal Alcohol Syndrome
Facial Malformations in Fetal Alcohol Syndrome
 Patient with DiGeorge syndrome. Note low set ears and wide set downward slanting eyes; often these ...
Patient with DiGeorge syndrome. Note low set ears and wide set downward slanting eyes; often these ...
 Down syndrome
Down syndrome
 Risk of Down Syndrome (Trisomy 21) by Maternal Age
Risk of Down Syndrome (Trisomy 21) by Maternal Age