A client is placed on fluid restrictions because of chronic kidney disease (CKD). Which assessment finding would alert the nurse that the client's fluid balance is stable at this time?
a. Decreased calcium levels
b. Increased phosphorus levels
c. No adventitious sounds in the lungs
d. Increased edema in the legs
Question 2
A client with chronic kidney disease (CKD) is experiencing nausea, vomiting, visual changes, and anorexia. Which action by the nurse is best?
a. Check the client's digoxin (Lanoxin) level.
b. Administer an anti-nausea medication.
c. Ask if the client is able to eat crackers.
d. Get a referral to a gastrointestinal provider.

 Assessment of coordination: heel slide.
Assessment of coordination: heel slide.
 Kidney Stone
Kidney Stone
 oral disease in aids
oral disease in aids
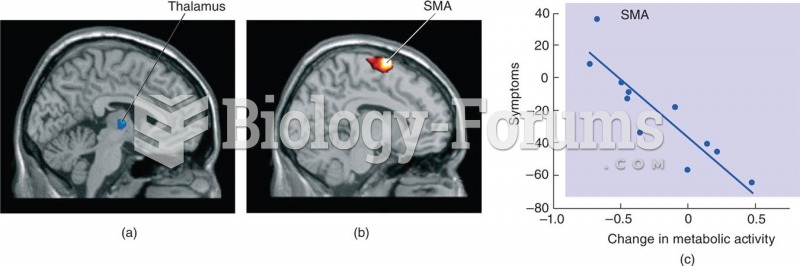 Gene Therapy of Parkinson’s Disease
Gene Therapy of Parkinson’s Disease
 Crohn's Disease
Crohn's Disease
 A deer tick can cause Lyme disease.
A deer tick can cause Lyme disease.