CHEST X-RAY AND ISOTOPE BONE SCAN
HISTORY: Patient with recurrent breast cancer, known (1)________ metastasis and increased alkaline (2)________.
INTERPRETATION: The chest x-ray shows (3)________ curvature of the thoracolumbar spine. Heart size is normal. Lung fields are clear. There is a metal (4)________ at the right base. The findings are unchanged from the 1990 film and no metastasis or effusion is identified.
An isotope bone scan following 24 millicuries of technetium 99 m Osteolite shows a prominent and intense pattern of (5)________ uptake that represents a change in comparison to the April 1990 film. Intensity of calvarial uptake is considerably higher than the facial bones and cervical spine, and shows a slightly (6)________ pattern. The patient has not had any intervening radiation therapy, and I think that these findings are suspicious for metastatic involvement in the calvaria. There is some increased (7)________ to the thoracolumbar spine related to the patient's scoliosis and unchanged from the 1990 film. The remainder of the skeleton, including the ribs, pelvis and extremities, is stable and unremarkable.
IMPRESSION: Chest shows scoliotic curvature unchanged from the 1990 film, with clear lungs and showing no evidence of (8)________ disease.
Isotope bone scan shows that since 1990, the patient has developed (9)________ increased calvarial uptake that has a slightly mottled pattern and is highly suspicious for metastatic disease to the calvaria. The remainder of the bone scan is stable, showing scoliosis and secondary increased uptake through the thoracolumbar spine, but no other specific bone (10)________ of metastatic disease are identified.
Question 2
DISCHARGE DIAGNOSES:
1. (1)________, malignant, laryngeal primary.
2. Alcoholic liver disease.
3. History of alcohol abuse.
4. Chronic obstructive pulmonary disease.
5. (2)________.
6. Malnutrition.
PROCEDURES PERFORMED: Total laryngectomy with right (3) ________ neck dissection.
COMPLICATIONS: None.
HOSPITAL COURSE: The patient was admitted for a total laryngectomy and neck (4)________ for treatment of a laryngeal carcinoma. Preoperatively, this was thought to be a T4N0 transchorionic carcinoma. The procedure was performed without complication. Postoperatively the patient did relatively well and was without significant pulmonary complications, although she did have respiratory therapy treatment throughout her hospital course. She was noted to have a low hematocrit and received 2 units of packed red blood cells. She was also noted to have a low magnesium level, and this was treated with (5)________ magnesium. The drains were removed on the 3rd postoperative day. She was noted to have some redness and erythema of the neck skin and was (6)________ treated with ampicillin and gentamicin for a possible infection. Further signs of infection were not noted other than a low-grade fever. She did not develop any (7)________ and was noted to be feeling well at the time. The nasogastric tube was discontinued on the 11th postoperative day. A (8)________ swallow was obtained prior to discontinuing the nasogastric tube and no (9)________ of the neck was noted. The patient tolerated tube feedings relatively well while the nasogastric tube was in place and once the tube was removed, she tolerated oral feedings well.
DISPOSITION:
1. The patient was discharged home without complications or problems.
2. Her diet and activity level should be as tolerated.
DISCHARGE MEDICATIONS: Tylenol with codeine (10)________ 30 mL p.o. q.4 hours p.r.n. One pint was dispensed.
FOLLOWUP:
1. Followup will be in the ENT clinic for suture removal.
2. The patient will also be followed by Speech Therapy as an outpatient and will receive radiation therapy treatments approximately 1 month postoperatively.

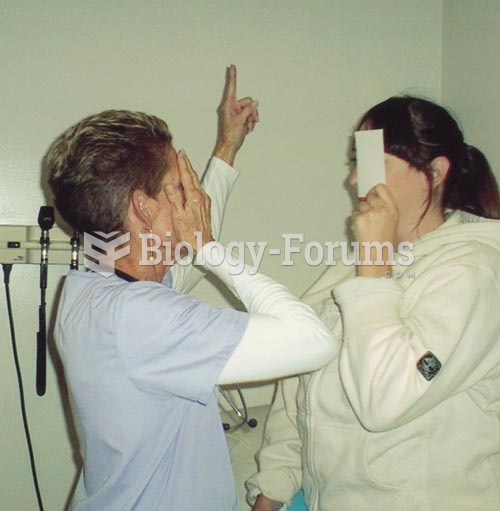 Testing Visual Fields by Confrontation: The nurse and patient should be approximately at an eye to e
Testing Visual Fields by Confrontation: The nurse and patient should be approximately at an eye to e
 Prostate cancer
Prostate cancer
 A Patient Being Prepared for Electroconvulsive Therapy.
A Patient Being Prepared for Electroconvulsive Therapy.
 ROM exercises on a patient’s wrist: radial deviation.
ROM exercises on a patient’s wrist: radial deviation.
 Chest x-ray of lung cancer; cancer is seen on the left side.
Chest x-ray of lung cancer; cancer is seen on the left side.
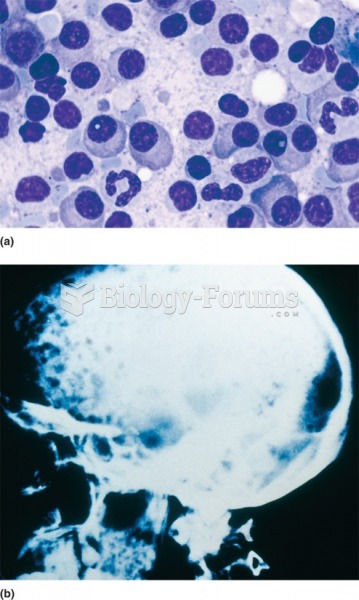 (a) Multiple myeloma: Tumor of plasma cells. (b) Myeloma cells grow within the bone and lesions can ...
(a) Multiple myeloma: Tumor of plasma cells. (b) Myeloma cells grow within the bone and lesions can ...