Answer to Question 1
Correct Answer: 1
Rationale 1: Bleeding with a placenta previa is a complication that can be life-threatening to both the mother and baby. This patient is the highest priority.
Rationale 2: Late decelerations are an abnormal finding, but put only the fetus at risk. This patient is not the highest priority.
Rationale 3: Grade I abruptio placentae creates slight vaginal bleeding. The urge to push indicates that delivery is near. This patient is not the highest priority.
Rationale 4: Although pregnancy-induced hypertension puts a woman at risk for developing abruptio placentae, there is no indication that this patient is experiencing this complication. This patient is not the highest priority.
Answer to Question 2
Correct Answer: 2,3
Rationale 1: Diabetes, multiparity, and preterm labor do not cause the same release of thromboplastin that triggers DIC.
Rationale 2: Abruptio placentae leave intrauterine arteries open and bleeding. This results in release of thromboplastin into the maternal blood supply and triggers the development of DIC. In prolonged retention of the fetus after demise, thromboplastin is released from the degenerating fetal tissues into the maternal bloodstream, which activates the extrinsic clotting system. This triggers the formation of multiple tiny clots, which deplete the fibrinogen and factors V and VII, and result in DIC.
Rationale 3: Abruptio placentae leave intrauterine arteries open and bleeding. This results in release of thromboplastin into the maternal blood supply and triggers the development of DIC. In prolonged retention of the fetus after demise, thromboplastin is released from the degenerating fetal tissues into the maternal bloodstream, which activates the extrinsic clotting system. This triggers the formation of multiple tiny clots, which deplete the fibrinogen and factors V and VII, and result in DIC.
Rationale 4: Diabetes, multiparity, and preterm labor do not cause the same release of thromboplastin that triggers DIC.
Rationale 5: Diabetes, multiparity, and preterm labor do not cause the same release of thromboplastin that triggers DIC.

 C, A nurse can also administer the medication by setting the dose and rate with an electronic infusi
C, A nurse can also administer the medication by setting the dose and rate with an electronic infusi
 It is important to act concerned when a patient is upset.
It is important to act concerned when a patient is upset.
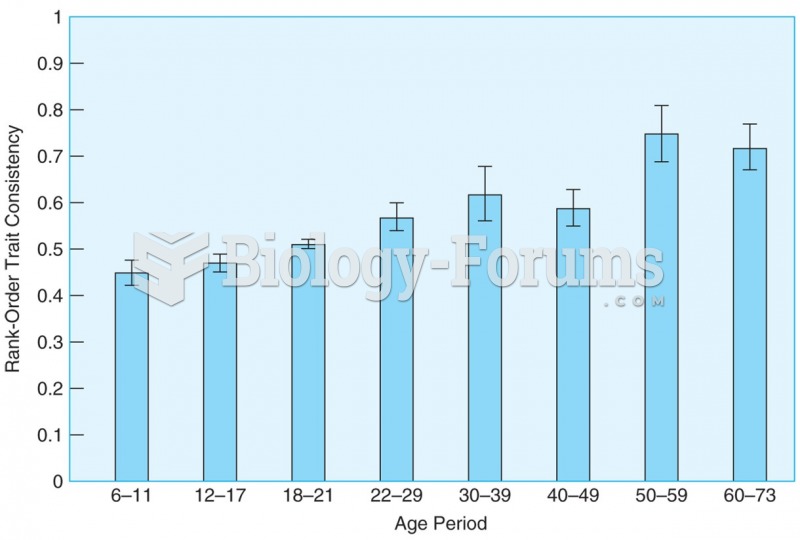 Rank-order correlations show that differential consistency remains high from childhood through late ...
Rank-order correlations show that differential consistency remains high from childhood through late ...
 How to plot a sine function with a negative amplitude and phase shift (Question 3 of 3)
How to plot a sine function with a negative amplitude and phase shift (Question 3 of 3)
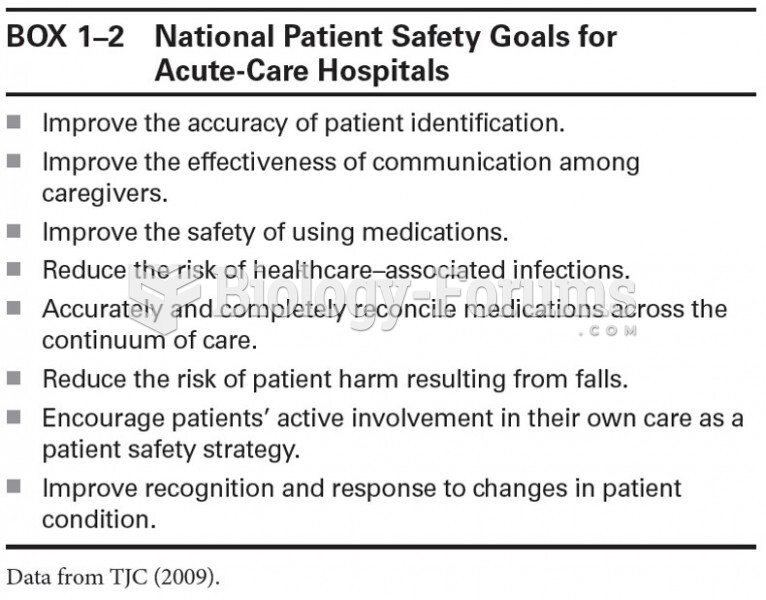 National Patient Safety Goals for Acute-Care Hospitals
National Patient Safety Goals for Acute-Care Hospitals
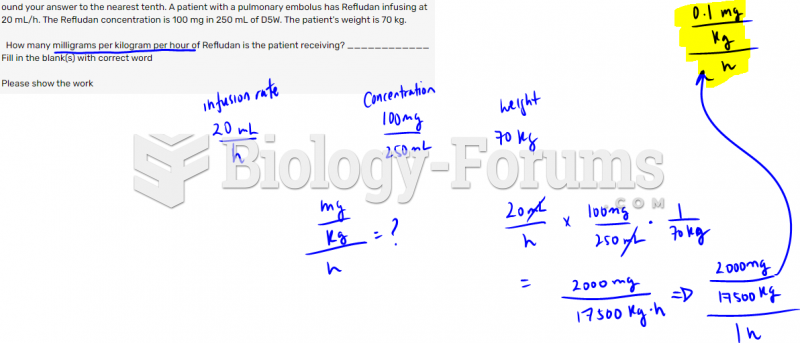 Round your answer to the nearest tenth. A patient with a pulmonary embolus has Refludan ...
Round your answer to the nearest tenth. A patient with a pulmonary embolus has Refludan ...