Answer to Question 1
ANS: A
Cervical assessment estimates whether the cervix is favorable for induction. The Bishop scoring system is used to estimate cervical readiness for labor with five factorscervical dilation, effacement, consistency, position, and fetal station. Vaginal birth is more likely to result if the Bishop score is higher than 8. This patient's Bishop score is low and she is at increased risk for an operative birth. Titration of Pitocin is at the judgment of the RN. A slower infusion of Pitocin allows more time for her body to adapt to the Pitocin and increases her potential for a nonoperative birth. Pitocin is a rapid-acting drug with an onset of 1 minute, duration of 30 minutes, and a half-life of 12 to 17 minutes. Cervical assessment is completed on an as-needed basis and is not scheduled. Assuring fetal well-being is important and can be determined by variability in the FHR baseline. A reactive nonstress test is not necessary prior to infusion. Establishing a baseline FHR prior to induction is a standard of care.
Answer to Question 2
ANS: D
A prior cesarean birth alone is not an indication for another cesarean birth for most women. Many women will choose repeat cesarean rather than a trial of labor even if they are appropriate candidates for VBAC because of the small, but real, added risk for uterine rupture. For other women, trying to deliver their next baby vaginallywhether successful or notis important to them. Cephalopelvic disproportion is a condition in which fetal size exceeds the size of the pelvis. In cases of true CPD, the probability of the second fetus being smaller is slim and a repeat cesarean section is warranted. The remaining indications for the primary cesarean section do not relate to fetal size and a VBAC may be considered.

 Photograph of an occupational therapist assisting a patient with learning independence in activities
Photograph of an occupational therapist assisting a patient with learning independence in activities
 Providing patient education
Providing patient education
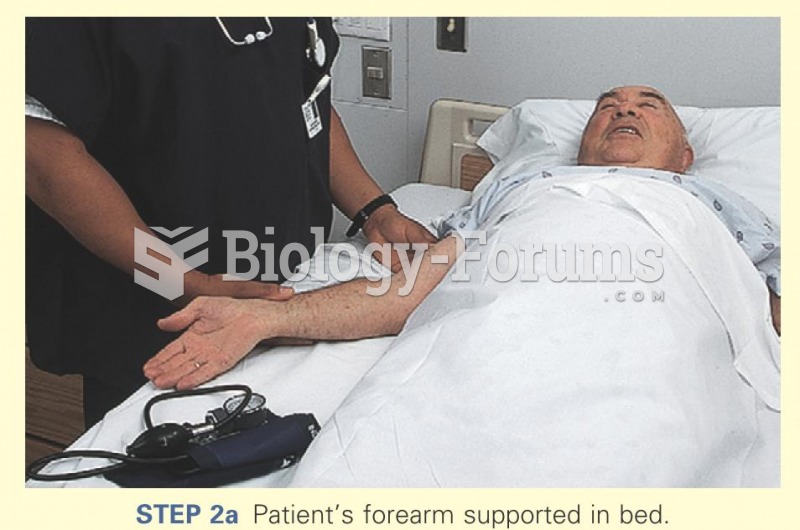 Patient's forearm supported in bed
Patient's forearm supported in bed
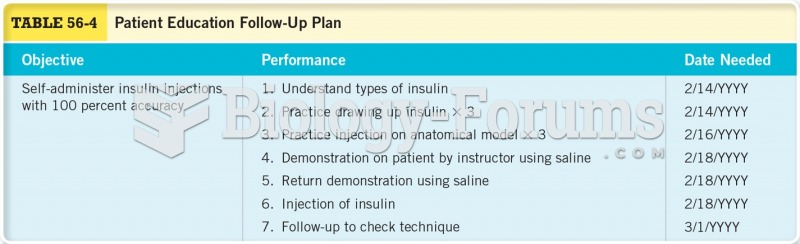 Patient Education Follow-up Plan
Patient Education Follow-up Plan
 Functional foods are being used by some health care professionals
Functional foods are being used by some health care professionals
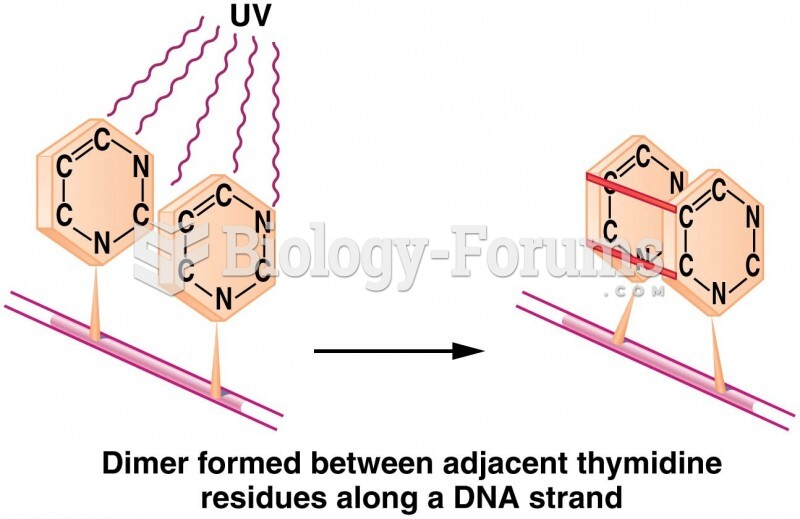 Induction of a thymine dimer by UV radiation, leading to distortion of the DNA
Induction of a thymine dimer by UV radiation, leading to distortion of the DNA