Answer to Question 1
To make medicine in the United States more scientific and more profitable, the Carnegie Foundation (at the request of the American Medical Association and the forerunner of the Association of American Medical Colleges) commissioned an official study of medical education. The Flexner report that resulted from this study has been described as the catalyst of modern medical education. To conduct his study, Abraham Flexner met with the leading faculty at the Johns Hopkins University School of Medicine to develop a model of how medical education should take place; he next visited each of the 155 medical schools then in existence, comparing them with the model. As a result of the Flexner report, all but two of the African American medical schools then in existence were closed, and only one of the medical schools for women survived. As a result, white women and people of color were largely excluded from medical education for the first half of the twentieth century. The Flexner report did help professionalize medicine. When we compare post-Flexner medicine with the characteristics of professions, we find that it meets those characteristics: (1) abstract, specialized knowledge, (2) autonomy, (3) self-regulation,
(4) authority, and (5) altruism.
Throughout its history in the United States, medical care has been on a fee-for-service basis. Patients are billed individually for each service they receive, including treatment by doctors, laboratory work, hospital visits, prescriptions, and other health-related expenses. There are both good and bad sides to the fee-for-service approach. The good side is that in the true spirit of capitalism, coupled with the hard work and scholarship of many people, this approach has resulted in remarkable advances in medicine. The bad side of fee-for-service medicine is its inequality of distribution. In effect, the United States has a two-tier system of medical care. Those who can afford it are able to get good medical treatment.
Answer to Question 2
False

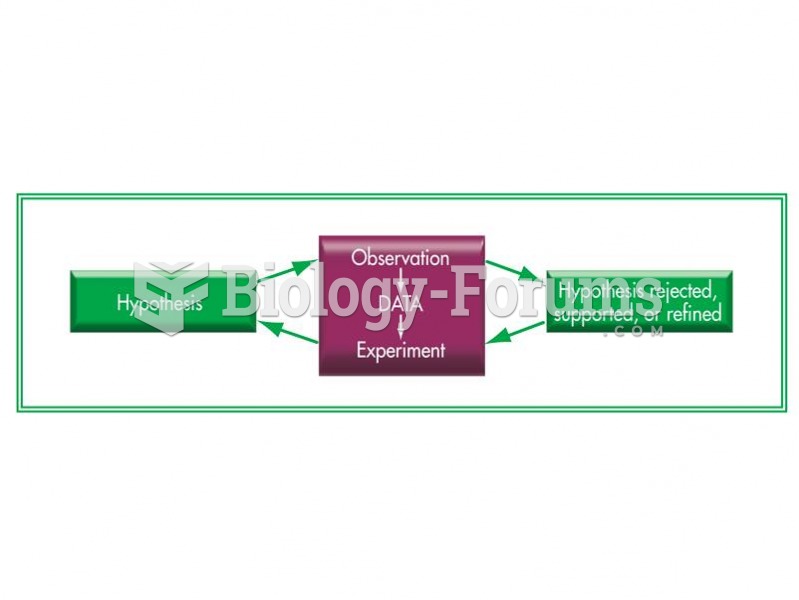 The scientific method.
The scientific method.
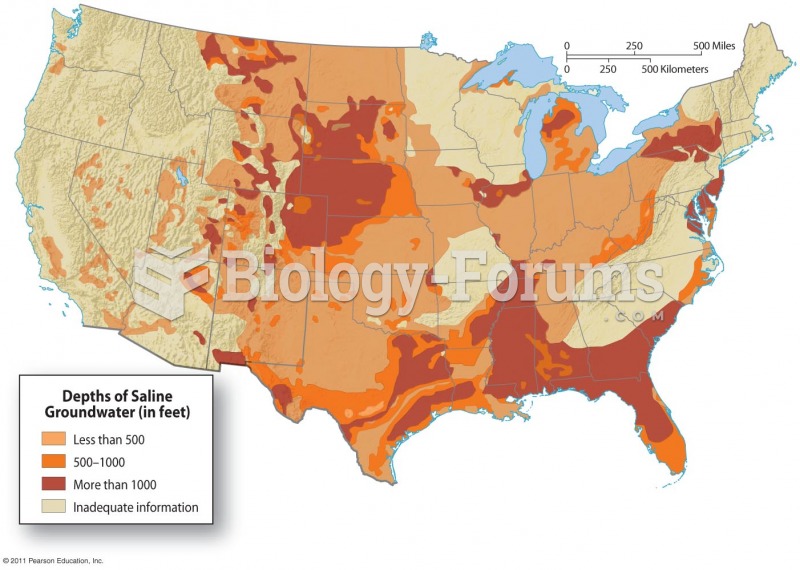 Saline Groundwater in the United States
Saline Groundwater in the United States
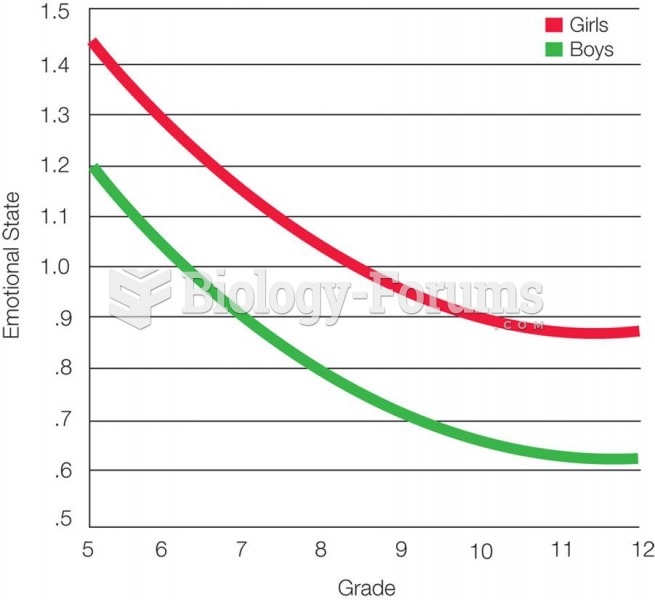 Change in Emotional States During Adolescence Average emotional state becomes teadilyi more negativ
Change in Emotional States During Adolescence Average emotional state becomes teadilyi more negativ
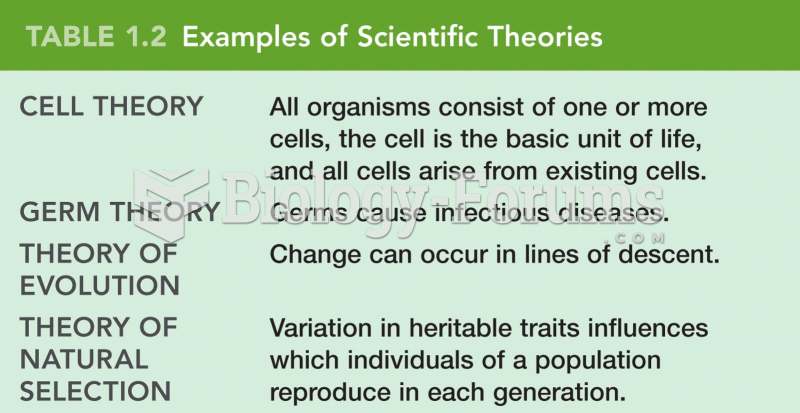 Examples of Scientific Theories
Examples of Scientific Theories
 Nutrias native to South America are abundant in freshwater marshes of the Gulf States. Their populat
Nutrias native to South America are abundant in freshwater marshes of the Gulf States. Their populat
 Regulatory effects of the vascular endothelium in normal and pathologic states
Regulatory effects of the vascular endothelium in normal and pathologic states