Answer to Question 1
ANS: C
A. Incorrect response: During ASV, the ventilator (1) uses the initial ventilator settings (i.e., high-pressure alarm, PEEP, and Fio2), (2) calculates system compliance, airway resistance, and auto-PEEP, and (3) uses the pressure limit of both mandatory and spontaneous breaths to determine the target breath and tidal volume.
B. Incorrect response: The therapist can adjust the rise time and the flow-cycling criterion.
C. Correct answer: The ventilator adjusts the I:E ratio and the inspiratory time of the mandatory breaths to prevent air trapping. These adjustments are accomplished by calculating the patient's expiratory time constants, and maintaining sufficient expiratory time.
D. Incorrect response: Pressure support ventilation is not part of ASV.
Answer to Question 2
ANS: D
A. Incorrect response: Switching to PC-SIMV with PSV would have no influence on the magnitude of the patient's spontaneous tidal volume. All that would be accomplished by making this switch is substituting volume-control ventilation for pressure-control ventilation. This change would affect only the mandatory breaths.
B. Incorrect response: MMV enables the patient to breath spontaneously, and ensures that the patient receives a minimum minute ventilation initially set by the therapist. However, MMV is a stand-alone mode and is not used with PC-SIMV with PSV.
C. Incorrect response: Increasing the inspiratory rise time has the effect of lengthening the time required for the pressure to reach its target value. Increasing the inspiratory rise time inappropriately can produce an increased work of breathing for the patient. Conversely, decreasing the inspiratory rise time too much can cause pressure overshoot, which contributes to premature cycling.
D. Correct response: Changing the flow-cycle criterion from 40 to 25 during PSV lengthens the inspiratory time and increases the tidal volume. Conversely, if the flow-cycle criterion is changed from 5 to 50, for example, the inspiratory time shortens and the tidal volume decreases. For ventilators lacking the flow-cycle criterion function, the therapist will increase the PSV level.

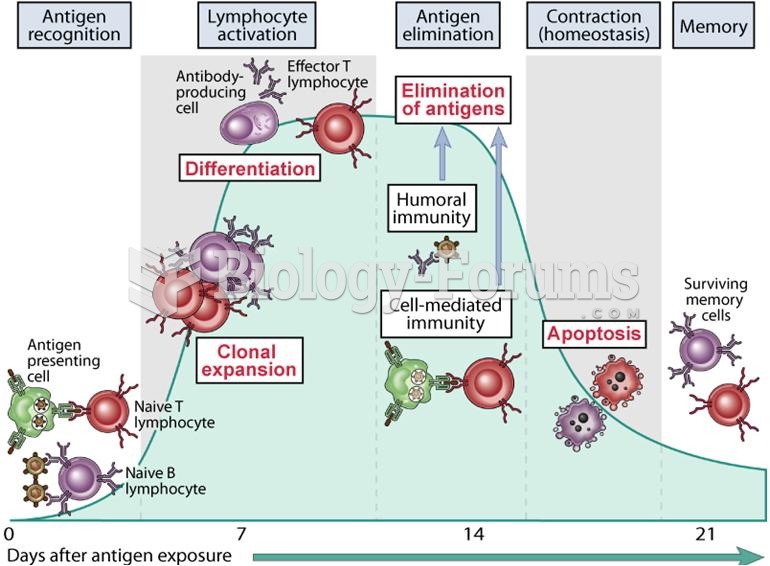 Phases of adaptive immune responses
Phases of adaptive immune responses
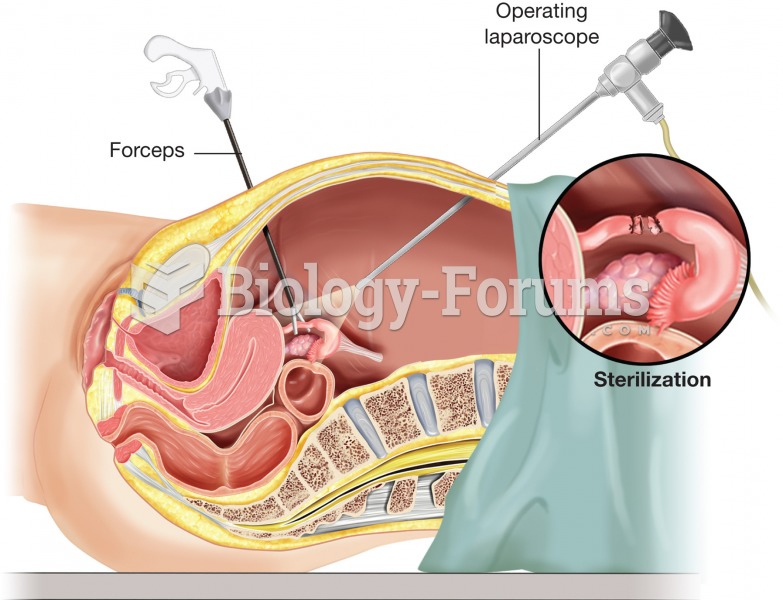 Tubal ligation. To minimize the size of the incisions necessary, laparoscopic surgery may be used to
Tubal ligation. To minimize the size of the incisions necessary, laparoscopic surgery may be used to
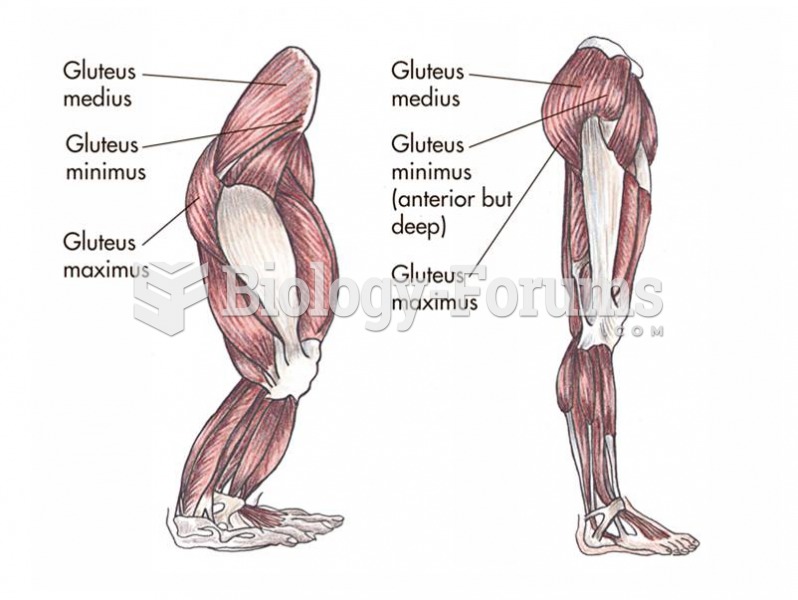 The gluteal muscles are repositioned in the biped and aid in support.
The gluteal muscles are repositioned in the biped and aid in support.
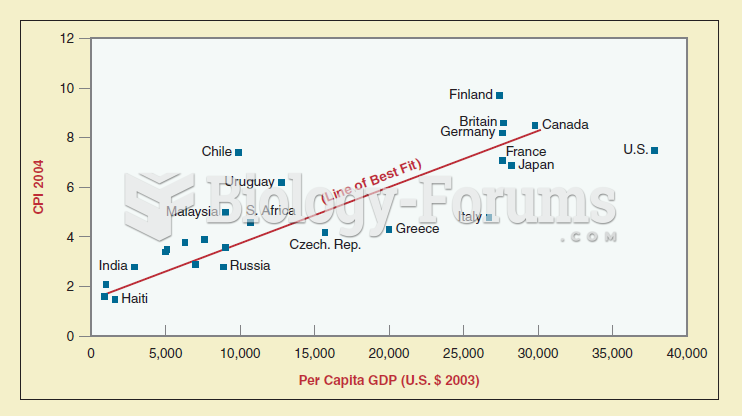 Scattergrams are a mechanism used by political scientists to show patterns and relationships among v
Scattergrams are a mechanism used by political scientists to show patterns and relationships among v
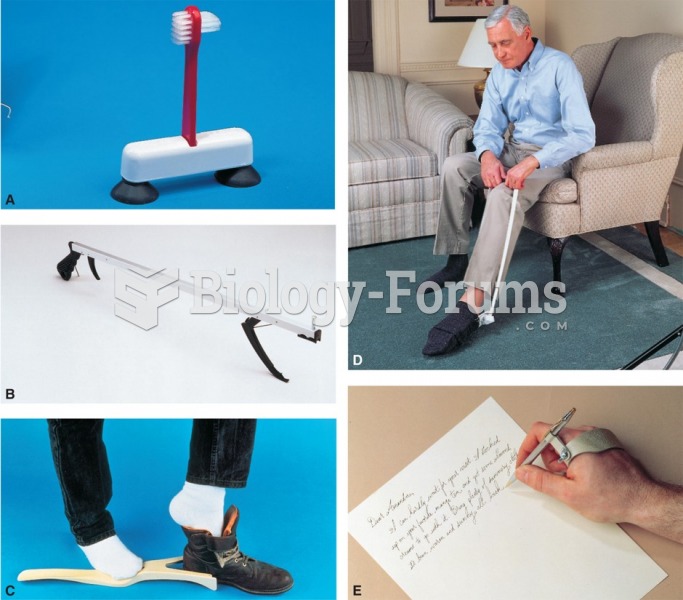 There are many types of adaptive devices: (A) a toothbrush; (B) a reaching stick; (C) a shoe holder; ...
There are many types of adaptive devices: (A) a toothbrush; (B) a reaching stick; (C) a shoe holder; ...
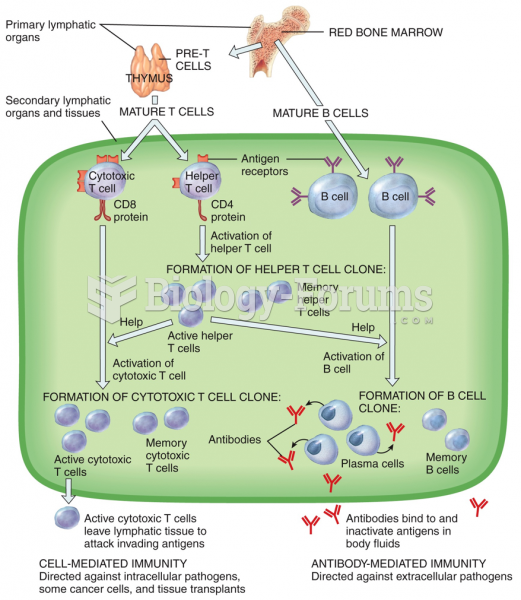 Adaptive Immunity
Adaptive Immunity