Answer to Question 1
ANS: B
Excerpts from the AARC guideline (CPG 36-4) include indications, contraindications, hazards and complications, assessment of need, assessment of outcome, and monitoring.
Answer to Question 2
ANS: D
Step 1: Assess Patient for Indications. Generally, a patient should never be suctioned according to a preset schedule. Although very thick secretions may not move with airflow and may not cre-ate any adventitious sounds, the patient should be assessed for clinical indicators, such as rhonchi heard on auscultation, which suggest the need for suctioning Step 2: Suction the Endotracheal Tube and Pharynx to Above the Cuff. Suctioning before extubation helps prevent aspiration of secretions after cuff deflation. After use, dispose of the first suction kit and prepare another for use, or prepare a rigid tonsillar (Yankauer) suction tip. Because patients will often cough after the tube is pulled, you may need to help them clear secretions.
Step 3: Oxygenate the Patient Well After Suctioning. Extubation is a stressful procedure that can cause hypoxemia and unwanted cardiovascular side effects. Administer 100 oxygen for 1 to 2 min to help avoid these problems.
Step 4: Deflate the Cuff. Attach the 10 or 12 ml syringe to the pilot tubing. Withdraw the air from the cuff while applying positive pressure to direct any pooled secretions above the cuff up into the oropharynx where they can immediately be suctioned with the tonsillar suction tip. Lis-ten for an audible leak around the tube. If no audible leak is present reinflate the cuff and discuss with the physician how to proceed.

 Visual Acuity Testing: Assist the patient in occluding the eye.
Visual Acuity Testing: Assist the patient in occluding the eye.
 Building competency in patient centered care
Building competency in patient centered care
 Computerized Patient Record (CPR)
Computerized Patient Record (CPR)
 Jaundice seen in the eyes and the skin of a patient with hepatitis A.
Jaundice seen in the eyes and the skin of a patient with hepatitis A.
 Many hunger-relief programs work to provide food aid to needy nations
Many hunger-relief programs work to provide food aid to needy nations
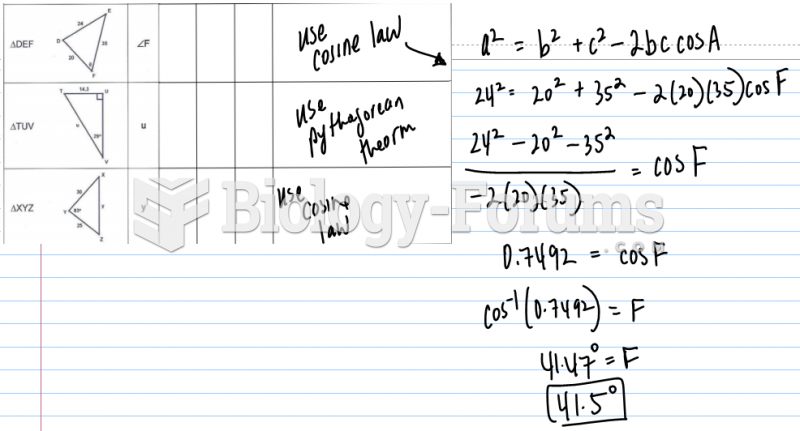 Provide the given and then write the formula and solve
Provide the given and then write the formula and solve