Answer to Question 1
ANS: B
Interpretation of the pulmonary function report: Interpretive strategies for pulmonary function testing abound. Most computer-based pulmonary function testing systems have algorithms in their software programs for computer-assisted interpretations of the pulmonary function report. A consensus for interpreting test results is growing. Table 20-8 summarizes pulmonary function changes that may occur in advanced obstructive and restrictive patterns of lung diseases, and Figure 20-16 presents a simple algorithm to assess pulmonary function test results in clinical prac-tice. When considering a pulmonary function report, the FEV1/VC ratio is a good place to start, because it provides an initial focus as normal, restrictive, or obstructive impairment. When the FEV1/FVC is less than the limit of normal (LLN), there is airway obstruction. When the FEV1/FVC is greater than the LLN, there is no airway obstruction. The LLN FEV1/FVC can be determined directly for various population using regression equations in Table 20-9 or simply estimated at 70. If the FEV1/FVC ratio is greater than the LLN or 70 and if the TLC is less than the LLN, often defined as less than 80 predicted normal, the patient has a restrictive im-pairment, according to this algorithm. The severity of the restriction is based on the percent pre-dicted or on the number of standard deviations below the LLN TLC according to Table 20-2. If the FEV1/FVC ratio is less than 70, the patient likely has an obstructive impairment; the se-verity of the obstruction is based on the percent predicted normal FEV1 according to Table 20-2. If the percent predicted normal DLCO is less than 80, the patient has a diffusion impairment. Some laboratories also report the DLCO/VA ratio, which indexes the DLCO for lung volume measured during the single breath test. If the DLCO/VA ratio is also less than 80 of the in-dexed value, the cause of the diffusion impairment is considered within the lung, and if the DLCO/VA ratio is greater than 80 of the indexed value, the cause of the diffusion impairment is considered due to small lung volume.
Answer to Question 2
ANS: D
Interpretation of the pulmonary function report: Interpretive strategies for pulmonary function testing abound. Most computer-based pulmonary function testing systems have algorithms in their software programs for computer-assisted interpretations of the pulmonary function report. A consensus for interpreting test results is growing. Table 20-8 summarizes pulmonary function changes that may occur in advanced obstructive and restrictive patterns of lung diseases, and Figure 20-16 presents a simple algorithm to assess pulmonary function test results in clinical prac-tice. When considering a pulmonary function report, the FEV1/VC ratio is a good place to start, because it provides an initial focus as normal, restrictive, or obstructive impairment. When the FEV1/FVC is less than the limit of normal (LLN), there is airway obstruction. When the FEV1/FVC is greater than the LLN, there is no airway obstruction. The LLN FEV1/FVC can be determined directly for various population using regression equations in Table 20-9 or simply estimated at 70. If the FEV1/FVC ratio is greater than the LLN or 70 and if the TLC is less than the LLN, often defined as less than 80 predicted normal, the patient has a restrictive im-pairment, according to this algorithm. The severity of the restriction is based on the percent pre-dicted or on the number of standard deviations below the LLN TLC according to Table 20-2. If the FEV1/FVC ratio is less than 70, the patient likely has an obstructive impairment; the se-verity of the obstruction is based on the percent predicted normal FEV1 according to Table 20-2. If the percent predicted normal DLCO is less than 80, the patient has a diffusion impairment. Some laboratories also report the DLCO/VA ratio, which indexes the DLCO for lung volume measured during the single breath test. If the DLCO/VA ratio is also less than 80 of the in-dexed value, the cause of the diffusion impairment is considered within the lung, and if the DLCO/VA ratio is greater than 80 of the indexed value, the cause of the diffusion impairment is considered due to small lung volume.


 Changes in boreal forest composition along a chronosequence in Quebec. Dates refer to the year of th
Changes in boreal forest composition along a chronosequence in Quebec. Dates refer to the year of th
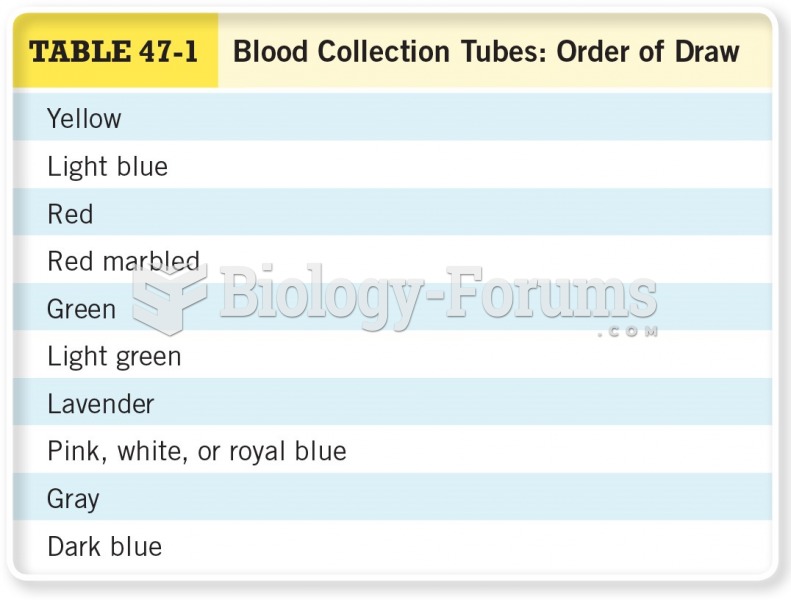 Blood Collection Tubes: Order of Draw
Blood Collection Tubes: Order of Draw
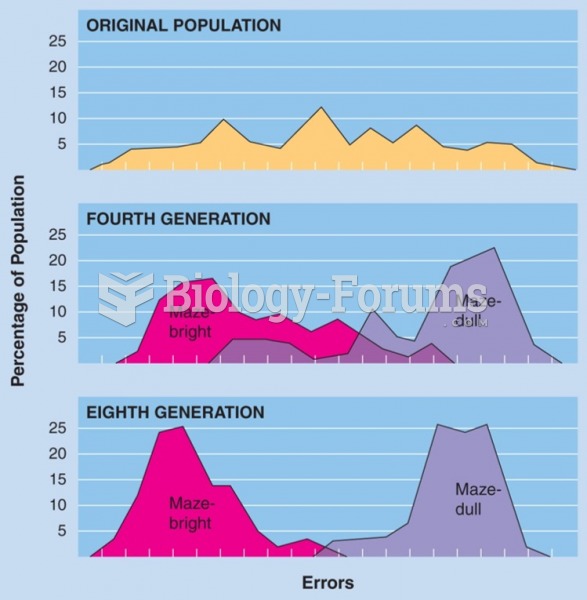 Selective breeding of maze-bright and maze-dull strains of rats by Tryon (1934). (Data from Cooper, ...
Selective breeding of maze-bright and maze-dull strains of rats by Tryon (1934). (Data from Cooper, ...
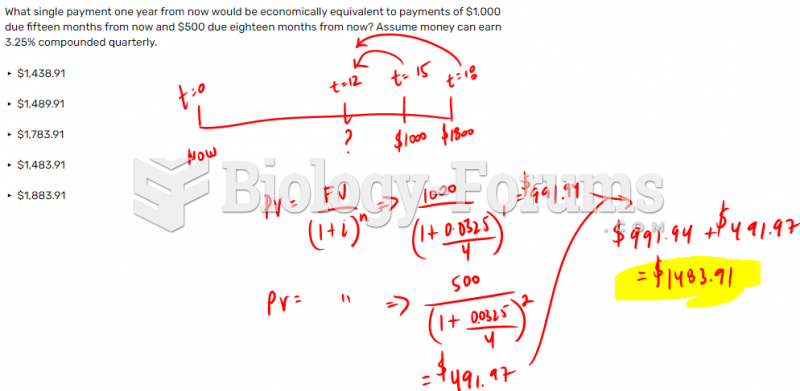 What single payment one year from now would be economically equivalent to payments of $1,000 ...
What single payment one year from now would be economically equivalent to payments of $1,000 ...
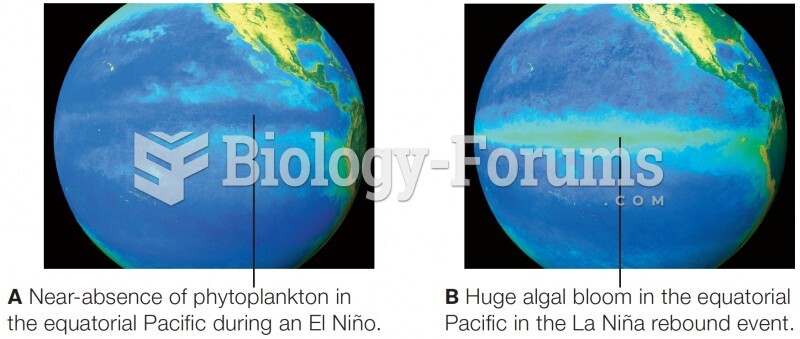 Satellite data on primary productivity in the equatorial Pacific Ocean
Satellite data on primary productivity in the equatorial Pacific Ocean
 Linkage Data from 39 Families with Cystic Fibrosis
Linkage Data from 39 Families with Cystic Fibrosis