Answer to Question 1
ANS: D
The medical record is a clinical data archive. The medical record serves as a tool for biomedical research and provider education, collection of statistical data for government and other agencies, maintenance of compliance with external regulatory bodies, and establishment of policies and regulations for standards of care. The record serves as the major communication tool between staff members and as a single data access point for everyone involved in the patient's care. It is a legal document that must meet guidelines for completeness, accuracy, timeliness, accessibility, and authenticity. The record can be used to assess quality-of-care measures, determine the medical necessity of health care services, support reimbursement claims, and protect health care providers, patients, and others in legal matters.
Answer to Question 2
ANS: D
The ANA's model for high-quality nursing documentation reflects the nursing process and includes accessibility, accuracy, relevance, auditability, thoughtfulness, timeliness, and retrievability. Standards for documentation are established by each health care organization's policies and procedures. They should be in agreement with The Joint Commission's standards and elements of performance, including having a medical record for each patient that is accessed only by authorized personnel. General principles of medical record documentation from the Centers for Medicare and Medicaid Services (2010) include the need for completeness and legibility; the reasons for each patient encounter, including assessments and diagnosis; and the plan of care, the patient's progress, and any changes in diagnosis and treatment.

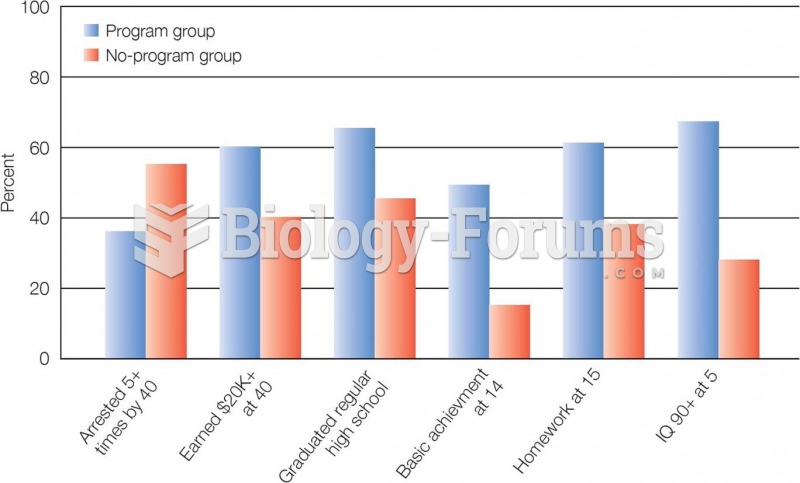 Major Findings of the High Scope Preschool Study High Scope participants showed better academic per
Major Findings of the High Scope Preschool Study High Scope participants showed better academic per
 Items that would be difficult to replace bearing legal significance are sent by certified mail.
Items that would be difficult to replace bearing legal significance are sent by certified mail.
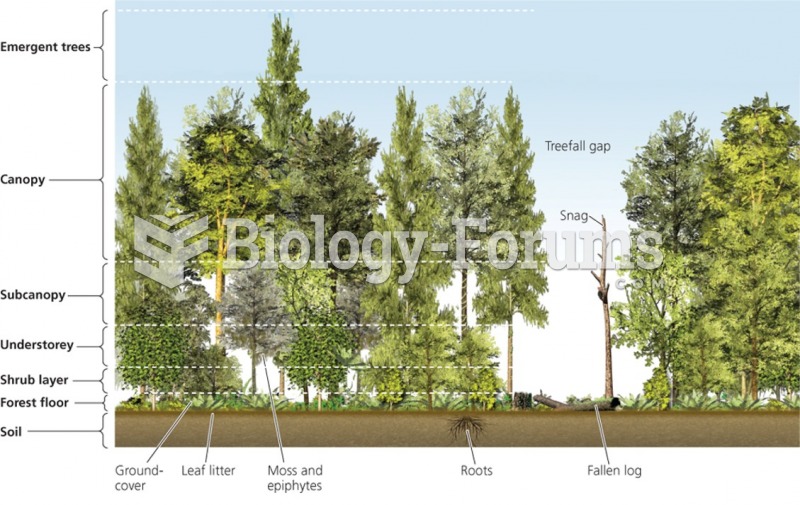 Major groups of forest biomes
Major groups of forest biomes
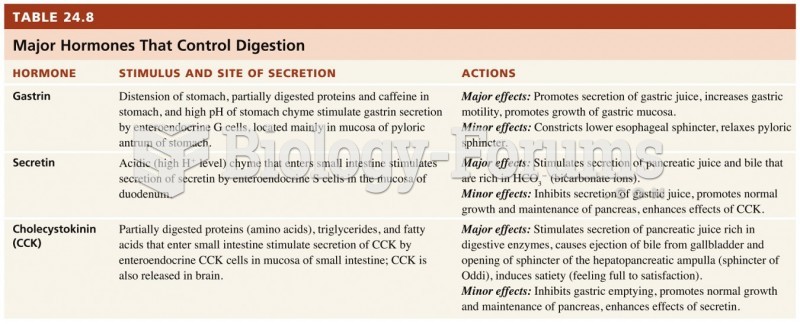 Major hormones
Major hormones
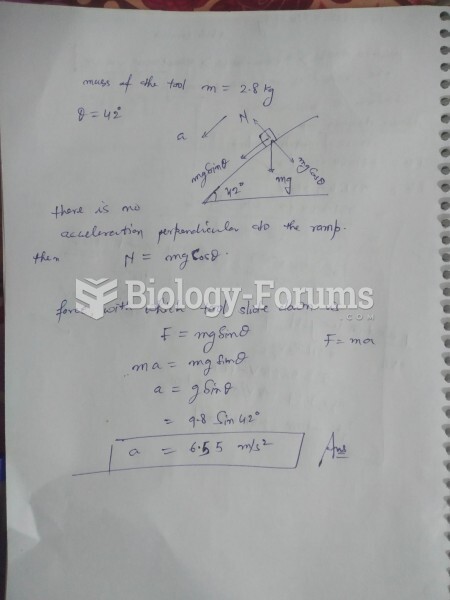 A 2.8-kg tool can move on a perfectly smooth ramp that slants at 42° above the horizontal. ...
A 2.8-kg tool can move on a perfectly smooth ramp that slants at 42° above the horizontal. ...
 Major RNA Molecules
Major RNA Molecules