Answer to Question 1
Correct Answer: 3
Rationale 1: Clients who have had previous AUCs are often able to self-diagnose.
Rationale 2: For women with AUC, follow-up usually consists of a routine office visit. No additional testing or cultures are necessary if the symptoms have promptly resolved.
Rationale 3: Clients whose symptoms have resolved quickly will be seen for a routine office visit.
Rationale 4: Most women with AUC will need to be seen for a follow-up visit; therefore, telling the client not to return unless symptoms return is incorrect.
Global Rationale: In many cases, a diagnosis of AUC is made by the health care provider based on symptoms and history alone, without additional serologic or urinary testing. Women who have experienced a prior AUC are often able to self-diagnose. Rapid dipstick tests are available to examine for the presence of infection. Follow-up of AUC is usually by routine office visit; no additional testing or cultures are required if the symptoms promptly resolve.
Answer to Question 2
Correct Answer: 1
Rationale 1: Switching from spermicidal foam to oral contraceptives might lessen this client's chances of having more AUCs.
Rationale 2: The cervical cap is similar to the diaphragm, and therefore would not lessen this client's chances of having AUCs.
Rationale 3: The use of spermicides or a diaphragm for contraception is a risk factor for AUC, so changing from a sponge filled with spermicides to a diaphragm would not be beneficial for this client.
Rationale 4: The female condom requires the use of spermicide, and the cervical cap is a smaller version of the diaphragm. Therefore, both forms of contraception would be risk factors for AUC.
Global Rationale: Use of spermicides or diaphragms for contraception increases risk of UTI. Changing from birth control methods such as cervical caps which are much like diaphragms and condoms and sponges that require spermicide may reduce incidence of UTI.

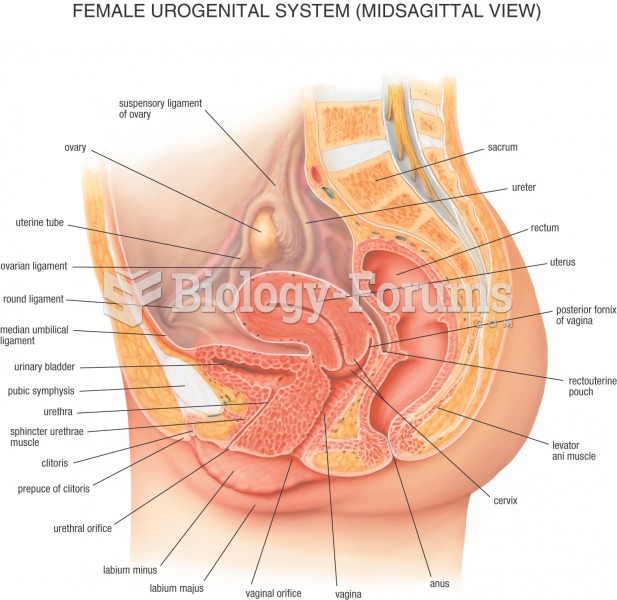 Female Anatomy
Female Anatomy
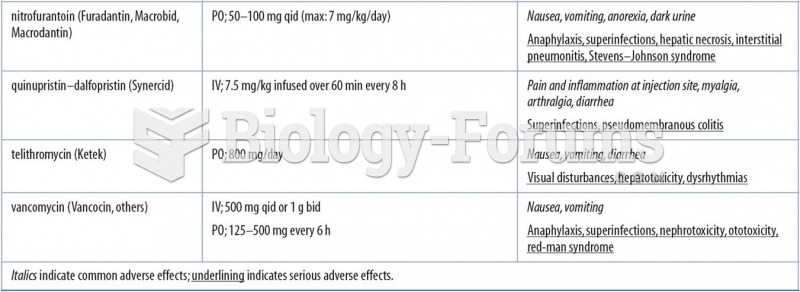 Selected Miscellaneous Antibacterials
Selected Miscellaneous Antibacterials
 Testing the client’s ability to feel vibrations, the knee
Testing the client’s ability to feel vibrations, the knee
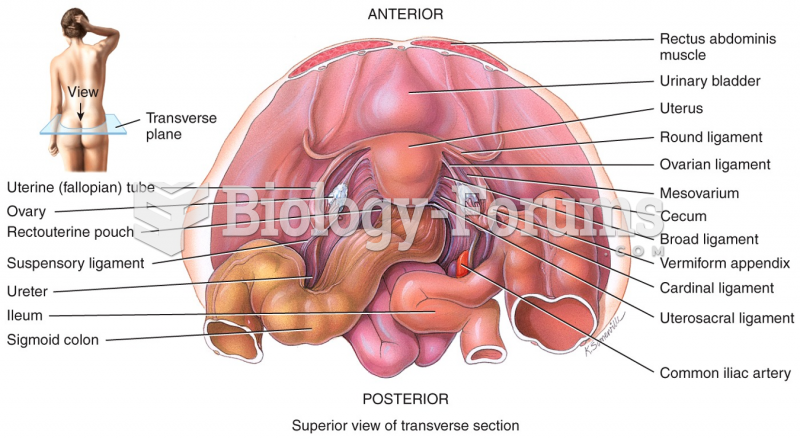 Female Reproductive System
Female Reproductive System
 A zebra orchid (Caladenia cairnsiana) mimics the scent of a female wasp
A zebra orchid (Caladenia cairnsiana) mimics the scent of a female wasp
 Vascular events in the acute inflammatory process
Vascular events in the acute inflammatory process