Answer to Question 1
Assessment data to observe: general appearance and behavior, poor skin turgor, decreased urinary output, sunken fontanel (in infant), decreased weight, increased pulse and respiration, decreased blood pressure, prolonged capillary refill.
Nursing diagnosis: altered nutrition-less than body requirements related to diarrhea losses and inadequate intake; fluid volume deficit related to excessive GI losses in stool or emesis.
Goals: child will maintain adequate hydration as evidenced by absence of above symptoms; child will maintain appropriate nutrition for age as evidenced by eating and retaining foods; child will not spread the infection to others; the family will receive appropriate support and education, especially home care and prevention.
Nursing interventions:
administer rehydration liquids, beginning with small amounts and gradually increasing to a regular diet; administer IV fluids as ordered; strict intake and output; weigh daily; assess vital signs, skin turgor, mucous membranes, mental status; discourage intake of carbonated beverages, fruit juices, and gelatin (these are high in carbohydrates, low in electrolytes, and have a high osmosis level); instruct family in providing appropriate therapy, monitoring intake and output, and assessing for signs of dehydration.
Answer to Question 2
The client will verbalize a desire to lose weight; acknowledge factors that have contributed to being overweight; understand some of the foods that she has eaten in the past are high in fat and cholesterol; improve her nutrition habits and eat a well-balanced diet; participate in an exercise program at least three times per week; lose 1 to 2 pounds weekly.

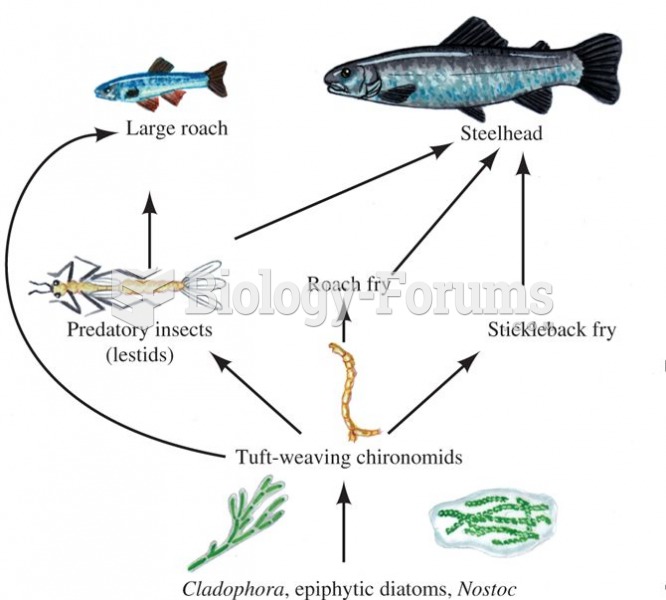 Food web associated with algal turf during the summer in the Eel River, California.
Food web associated with algal turf during the summer in the Eel River, California.
 Scorpion mother
Scorpion mother
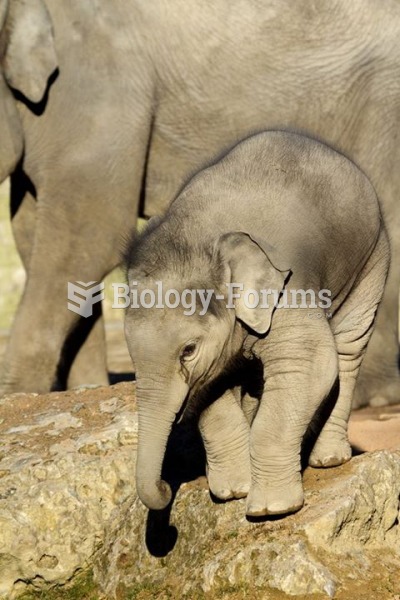 Baby elephant and its mother
Baby elephant and its mother
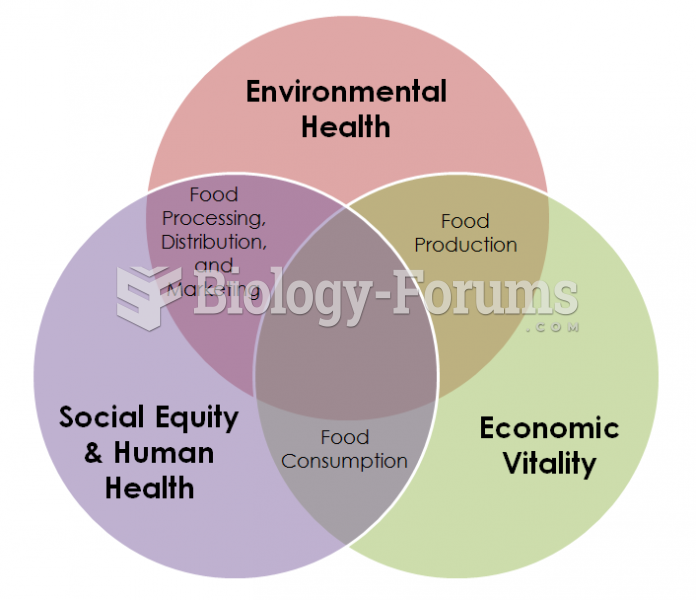 Sustainable Food Security
Sustainable Food Security
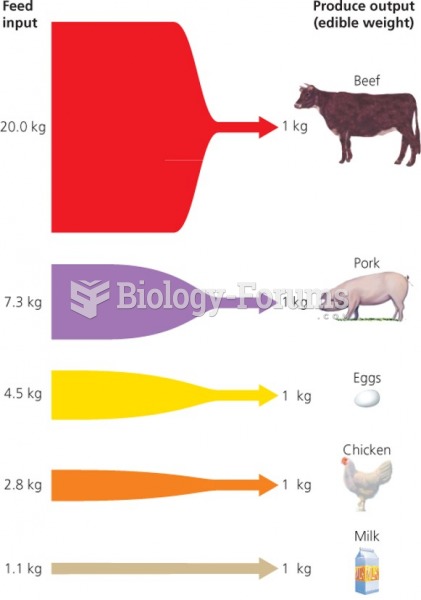 Food choices vs. energy choices
Food choices vs. energy choices
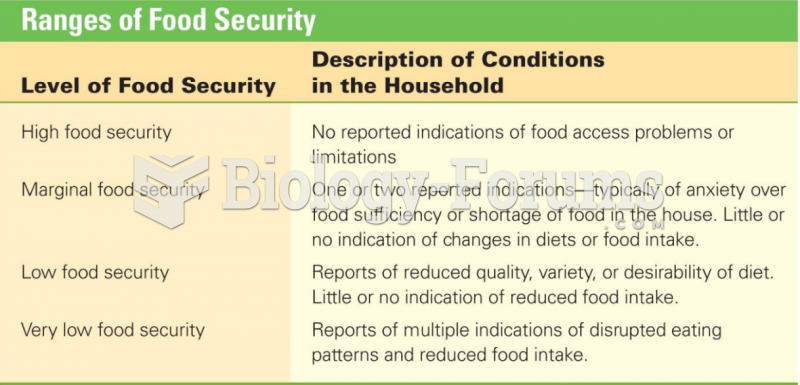 Ranges of Food Security
Ranges of Food Security