Answer to Question 1
Severe PEM encompasses a continuum of malnutrition: at the extremes are two distinct types of severe PEM, and between them conditions that combine features of both.
Marasmus is at one end of the continuum. It results from severe, chronic, overall malnutrition. In marasmus, fat and muscle tissue are depleted, and the skin hangs in loose folds, with the bones clearly visible beneath the skin. Children with marasmus tend at first to be alert and ravenously hungry, although with increasing severity they become apathetic and lose their appetites. Clinicians often say that marasmus represents the body's survival response to long-term, chronic dietary insufficiency.
Kwashiorkor is the other extreme type of PEM. It is often distinguished from marasmus by the presence of severe edema. While edema sometimes is present in children with marasmus, those with kwashiorkor usually have more extensive edema, which typically starts in the legs but often involves the entire body. Fluid accumulates in the abdominal cavity. Children with kwashiorkor sometimes have large, distended abdomens due to ascites. Because malnourished children often have intestinal parasites, worms sometimes contribute to this abdominal distension as well. Children with kwashiorkor often are apathetic and have cracked and peeling skin, enlarged fatty livers, and sparse unnaturally blond or red hair. Although many characteristics of kwashiorkor were once thought simply to be caused by protein deficiency, this does not appear to be the case. Researchers now believe that many of the signs and symptoms of kwashiorkor are the result of micronutrient deficiencies, for example vitamin A deficiency, in combination with infection or other environmental stressors.
Answer to Question 2
b

 For some Americans, religion is an “easy-going, makes-little-difference” matter, as expressed in ...
For some Americans, religion is an “easy-going, makes-little-difference” matter, as expressed in ...
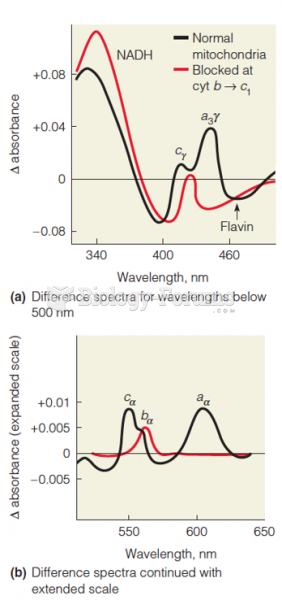 Difference spectra of mitochondria
Difference spectra of mitochondria
 There Is a Difference between Natural and Added Sugars
There Is a Difference between Natural and Added Sugars
 Difference-Between-Carbohydrates-and-Lipids-infographic
Difference-Between-Carbohydrates-and-Lipids-infographic
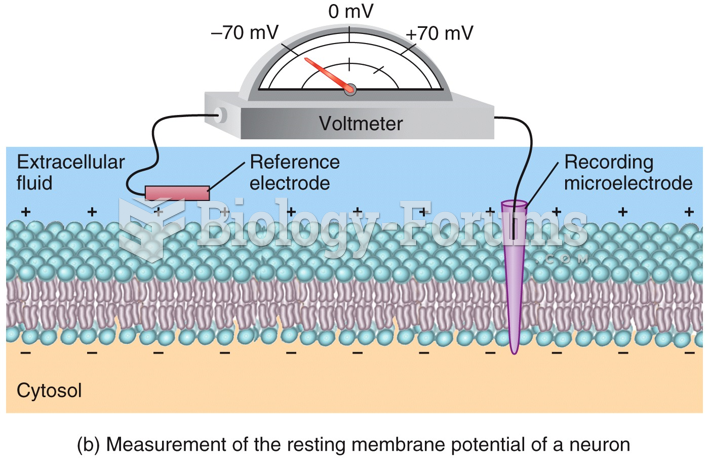 Resting Membrane Potential: Voltage Difference
Resting Membrane Potential: Voltage Difference
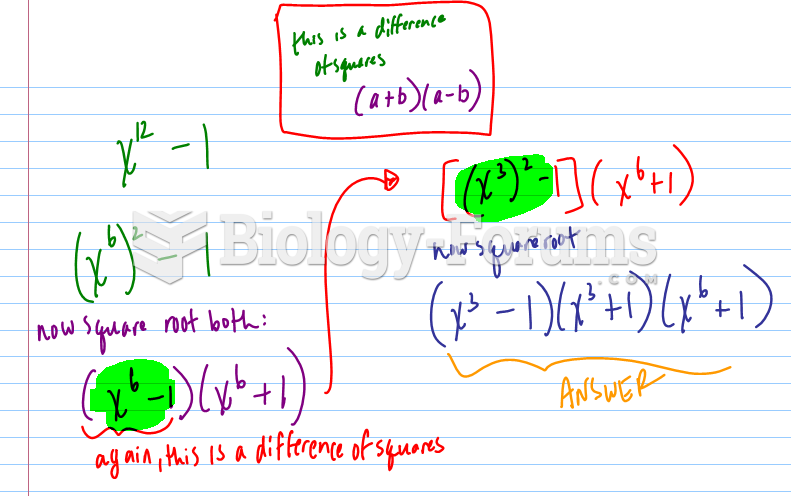 Difference of Squares
Difference of Squares