Answer to Question 1
The scarred tissue of a cirrhotic liver impedes the flow of blood, three-fourths of which is supplied by the hepatic portal vein. The restricted blood flow within the liver stimulates the release of vasodilators (and therefore, increased blood flow) in nearby arterioles, leading to a greater volume of portal blood. The increased portal blood coupled with resistance to blood flow within the liver causes a rise in blood pressure within the hepatic portal vein, called portal hypertension. As portal pressure builds, some of these collaterals can become enlarged and engorged with blood, forming varices. The varices that develop in the esophagus and stomach are vulnerable to rupture because they have thin walls and often bulge into the lumen. If ruptured, they can cause massive bleeding that is sometimes fatal. The blood loss is exacerbated by the liver's reduced production of blood-clotting factors. Within 10 years of disease onset, about 50 percent of cirrhosis patients develop ascites, a large accumulation of fluid in the abdominal cavity. Ascites is primarily a consequence of portal hypertension, sodium and water retention in the kidneys, and reduced albumin synthesis in the diseased liver. As a result of portal hypertension, the distorted blood flow elsewhere in the body alters kidney function, leading to sodium and water retention and an accumulation of body fluid. The elevated pressure within the liver's small blood vessels causes fluid to leak into lymphatic vessels and, ultimately, the abdominal cavity. The movement of water into the abdomen is exacerbated by low levels of serum albumin, a protein that helps to retain fluid in blood vessels.
Answer to Question 2
D

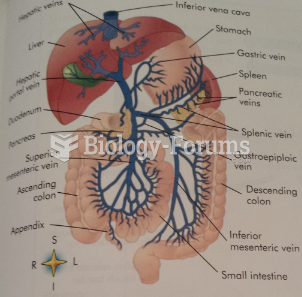 Hepatic Portal Circulation
Hepatic Portal Circulation
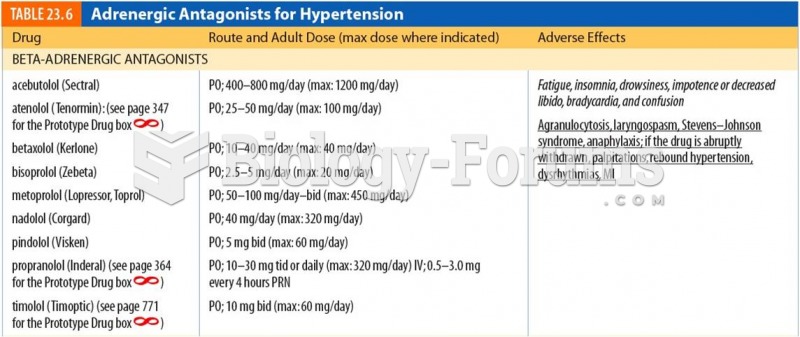 Adrenergic Antagonists for Hypertension
Adrenergic Antagonists for Hypertension
 Gislebertus, Last Judgment, tympanum and lintel, west portal, cathedral, Autun, France.
Gislebertus, Last Judgment, tympanum and lintel, west portal, cathedral, Autun, France.
 Central portal of the west facade, Reims Cathedral, France.
Central portal of the west facade, Reims Cathedral, France.
 Prolonged abuse leads to production of stress hormones that can lead to a cascade of effects ...
Prolonged abuse leads to production of stress hormones that can lead to a cascade of effects ...
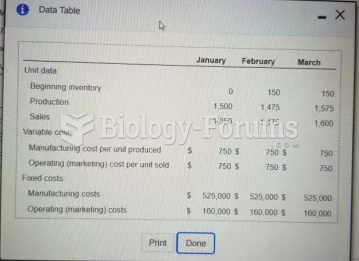 E9-23 Prepare income statements Explain the difference in operating income
E9-23 Prepare income statements Explain the difference in operating income