Answer to Question 1
Energy: 22-25 kcal/kg IBW to facilitate weight loss
1250 -1420 kcal
May also use Mifflin St. Jeor equation to determine energy requirements.
Protein: 0.8 g/kg body weight
0.8 g/kg x IBW (57 kg) = 45.6 . Increasing protein may help increase satiety and aid in weight reduction. 1.0 g/kg x 57 kg = 57 g.
46-57 g protein
Answer to Question 2
On day 4, the metabolic cart measured Mr. Perez's calorie expenditure to be 3657 kilocalories with an RQ value of 0.76 . On day 7, Mr. Perez received slightly more than ordered by his nutrition prescription (102): 199 grams protein and 3034 kcal. Compared to his metabolic cart, he was not meeting his needs by parenteral feeding alone. He received 83 of his energy needs, or 40 kcal/kg IBW and 2.6 grams protein/kg IBW. Based on these comparisons, Mr. Perez is on the higher end or is above his original recommendations for estimated energy and protein needs.
If necessary, it is possible to increase his protein intake through TPN. This would not only provide the patient with more energy, but it would also be beneficial for wound healing. It would also be beneficial to increase his energy intake, especially when he is no longer receiving propofol, because his RQ value indicates that the patient is closer to a fasting state. Increased carbohydrate intake can also increase the RQ value. Thus, increasing his CHO intake would match his energy expenditures more closely based on his metabolic cart measurement and cause the RQ value to represent a fed state. Since he is currently receiving propofol as a sedative, he is receiving 25 of his energy needs through the administration of this medication.
It is important to not overfeed the patient and to provide Mr. Perez with nutrition support at a level he can tolerate. Thus, there are several limitations that prevent the healthcare team from making significant changes to the nutrition support regimen, such as the patient's current mechanical ventilation. They will not want to increase carbohydrate content or risk overfeeding, which would interfere with weaning him off of the ventilator. Increasing the dextrose/carbohydrate in the TPN could also exacerbate his hyperglycemia . Also, the team may be hesitant to increase calories from fat because of the risk for continued hypertriglyceridemi a and liver dysfunction with liver lacerations. The medical team may not want to increase the risk for pressure changes due to the presence of edema by increasing the PN volume. Next, the medical team may not want to make significant changes to the nutrition support regimen related to the method of delivery because of the patient's anastomotic leak and previous GI tract discontinuity. In other words, an increase in enteral formula could cause pressure changes within the GI tract, as well as increase the risk for leakage. This could prevent the closure of the abdominal wound, which is the goal of the medical team at this time.

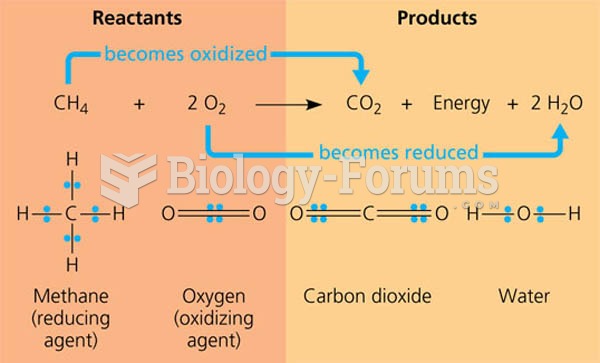 Methane combustion as an energy–yielding redox reaction.
Methane combustion as an energy–yielding redox reaction.
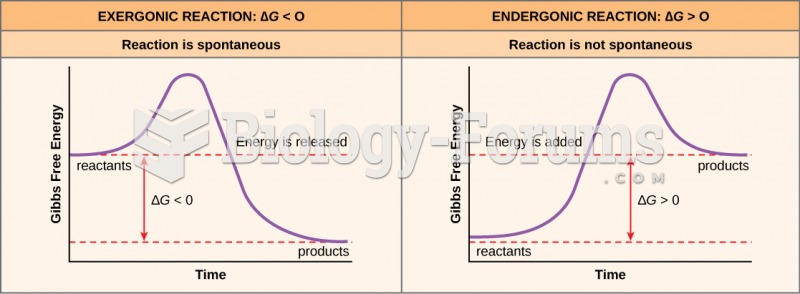 Free Energy Enzymes
Free Energy Enzymes
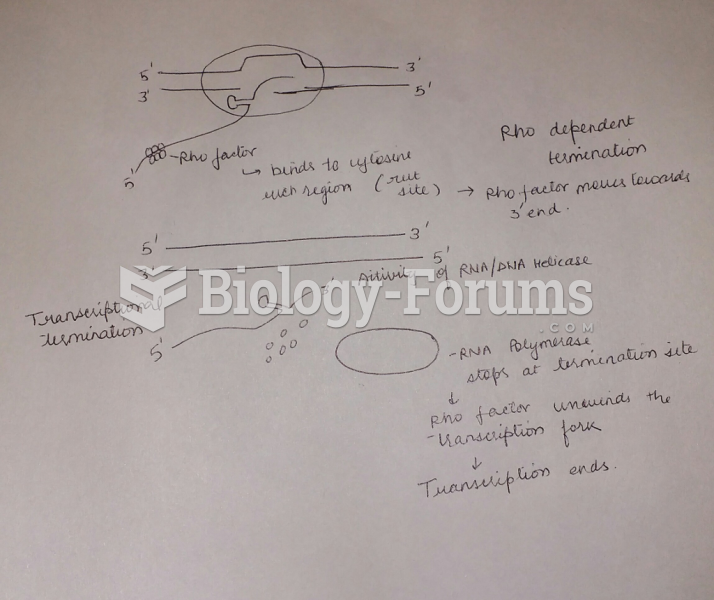 Draw and label a diagram and explain how a factor-dependent transcription (rho-dependent) terminator
Draw and label a diagram and explain how a factor-dependent transcription (rho-dependent) terminator
 Translation of an RNA message into a protein
Translation of an RNA message into a protein
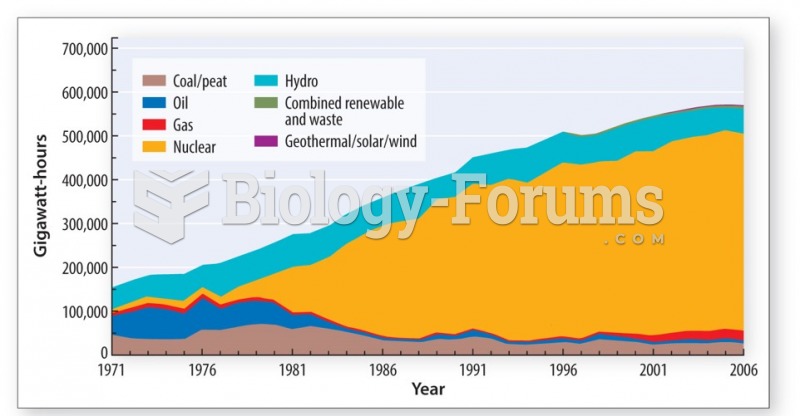 France has produced most of its energy from nuclear power since the oil crisis of the 1970s
France has produced most of its energy from nuclear power since the oil crisis of the 1970s
 The functional role of pRB. The pRB protein product of RB1
The functional role of pRB. The pRB protein product of RB1