Code the following cases for inpatient facility purposes using ICD-9-CM and ICD-10-CM and PCS codes.
Calculate the MS-DRG.
Identify the Principal vs. Secondary diagnoses and procedures.
Use external cause codes when appropriate.
Do NOT code procedures that are captured by the facility chargemaster.
Secondary diagnoses and procedures do NOT need to be sequenced in any particular order. Enter "None" when no code is required.
If more than one occurrence of a procedure is required, report the code with "x 2""x 3" etc.
INPATIENT HOSPITAL
Health Record Face Sheet
Record Number: 80-50-77
Age: 77
Gender: Female
Length of Stay: 5 Days
Service Type: Inpatient
Discharge Status: To Home Health
Diagnosis/Procedure: Peritrochanteric Right Hip Fracture
Mild Hypertension
Total Right Hip Arthroplasty
DISCHARGE SUMMARY
PATIENT: JOY INPATIENT
RECORD NUMBER: 80-50-77
ADMITTED: 09-15-XX
DISCHARGED: 09-20-XX
PHYSICIAN: DR. ALEX, M.D.
DISCHARGE DIAGNOSIS: Peritrochanteric right hip fracture.
Mild hypertension.
PROCEDURE(S): Total right hip arthroplasty.
HISTORY OF THE PRESENT ILLNESS: This is a 77-year-old white female who presented to the emergency room with complaint of pain in the right hip after falling down at her home. The patient slipped on the kitchen floor. She was not able to get up because of her complaints of right hip pain. She did not have any significant shortening of the right lower extremity but is very minimally externally rotated.
LABORATORY DATA: We obtained blood for CBC, chem screen, PT, PTT and a urinalysis. We did an EKG, which shows a normal sinus rhythm. There-are no acute ST or T-wave changes and a chest x-ray was also done which is not particularly remarkable, other than borderline cardiomegaly.
HOSPITAL COURSE: The patient was admitted to the hospital for definitive treatment of the right hip fracture in the form of a total hip arthroplasty. The patient was sent to the orthopedic floor and was provided immediate relief with routine fractured hip care orders. The patient was given pain medication in form of Mepergan 2 cc intramuscularly. IV was started and Foley catheter inserted in anticipation of emergent surgery and prior to being taken to the operating room. Patient tolerated the procedure well and was able to start physical therapy on day one after the surgery. Patient progressed slowly over the next couple of days but showed constant improvement. On day five, the patient was discharged to home with order for home health and physical therapy.
DISCHARGE PLANS: The patient will receive home health and physical therapy on a twice-weekly basis for six weeks. After 6 weeks, the patient will be re-evaluated.
DR. ALEX, M.D.
Electronically authenticated by Dr. Alex, M.D., 09-21-xx 445
HISTORY AND PHYSICAL
PATIENT: JOY INPATIENT
RECORD NUMBER: 80-50-77
ADMITTED: 09-15-XX
DISCHARGED: 09-20-XX
PHYSICIAN: DR. ALEX, M.D.
CHIEF COMPLAINT: Pain in the right hip after falling down at her home. The patient slipped on the kitchen floor.
HISTORY OF PRESENT ILLNESS: This 77-year-old white female was admitted following -a fall when she slipped on her apartment kitchen floor and fell down and injured her right hip. She was brought by ambulance from her home to the Emergency Room where she was evaluated. X-rays were obtained that showed a nondisplaced peritrochanteric fracture of the right hip. She was admitted and placed in Buck's traction and will be scheduled for surgery at the earliest convenience.
DRUG ALLERGIES: Percoset.
MEDICATIONS: Daily vitamin and Wytensin for hypertension.
FAMILY HISTORY: Noncontributory.
SOCIAL HISTORY: Lives alone with close neighbors and three children who all live in the same area and visit her regularly.
PAST MEDICAL HISTORY:
She has a history of mild hypertension and previous cholecystectomy as well as a melanoma removed from her left lower eyelid 10 years ago.
PHYSICAL EXAMINATION:
VITAL SIGNS: Temperature is 98.6, pulse 102, respirations 16, and blood pressure is 155/70.
GENERAL: This is a healthy and quite alert white female for age, no acute distress.
HEENT/NECK: Edentulous, has a skin graft in the left lower eyelid consistent with her melanoma surgery, wears glasses, otherwise within normal limits.
CARDIOVASCULAR: Clear. Heart slightly enlarged PMI at the anterior axillary line, no murmurs, regular rate and rhythm.
ABDOMEN: Protuberant, soft, well-healed abdominal scar.
EXTERMITIES: Right leg in a slightly externally rotated position. Distally pulses are palpable. There is no significant pitting edema.
GENITORECTAL: Genitalia and rectal deferred.
NEUROLOGICAL: Oriented times four. Cranial nerves II through XII intact. Deep tendon reflexes are symmetrical except the right leg, which was not tested.
DIAGNOSTIC STUDIES: X-rays were obtained that showed a nondisplaced peritrochanteric right hip fracture.IMPRESSION: Peritrochanteric right hip fracture.
RECOMMENDATIONS/PLAN: At this time, the patient is admitted for definitive care of her right hip. I discussed surgical versus conservative- management and because the patient is very active, she has opted for surgery. The patient is being admitted for a total hip arthroplasty. Risks of infection, pulmonary embolus, anesthetic risks, other treatment options and ramifications were discussed at length with the patient. She is understands these risks and wishes to proceed.
DR. ALEX, M.D.
Electronically authenticated by Dr. Alex, M.D., 09-15-xx 8876
OPERATIVE REPORT
PATIENT: JOY INPATIENT
RECORD NUMBER: 80-50-77
DATE OF SURGERY: 09-15-XX
SURGEON: DR. ALEX, M.D.
PREOPERATIVE DIAGNOSIS: Peritrochanteric right hip fracture.
POSTOPERATIVE DIAGNOSIS: Peritrochanteric right hip fracture.
OPERATIVE PROCEDURE: Total right hip arthroplasty, Ceramic-on-Polyethylene.
ANESTHESIA: General.
DESCRIPTION: After adequate sedation, the patient was brought to the operating room and placed in supine position on the operating table. After obtaining proper anesthesia, the patient was prepped and draped in the usual fashion for right hip arthroplasty. Incision was made along the posterior aspect of the right hip with the patient in a lateral decubitus position. The short external rotator muscles were released by incision from their insertion on the femur, exposing the joint capsule. The capsule was incised. The hip was then dislocated posteriorly. The femoral head was resected with a reciprocating saw. Osteophytes found around the rim of the acetabulum were removed with an osteotome. Acetabulum was then reamed out with power reamer exposing both subchondral and cancellous bone. The acetabular component was inserted with good result. The femoral canal was then prepared utilizing a hand reamer. A caliper was utilized to measure the femoral head size for replacement with appropriate component selected. The femoral shaft was prepared by enlarging the canal. The stem was secured into the femoral shaft and then pounded into place with an impactor. No complications were experienced and the stem secure. The femoral stem prosthesis was then reduced and repositioned. No allograft or auto graft was required. The external rotator muscles are reattached and the incision was sutured in multiple layers placement of four suction drains. Estimated blood loss was 340 cc. Autologous blood collection was done intraoperatively with transfusion of whole blood perioperative. Sponge and needle count were correct. Patient was sent to recovery in satisfactory condition.
DR. ALEX, M.D.
Electronically authenticated by Dr. Alex, M.D., 09-15-xx
ICD-9-CM diagnosis code(s): PDx_____________________
SDx _____________________
ICD-9-CM procedure code(s): PPx_____________________
SPx_____________________
ICD-10-CM diagnosis code(s): PDx_____________________
SDx _____________________
ICD-10-PCS procedure code(s): PPx_____________________
SPx_____________________
MS-DRG: _____________________

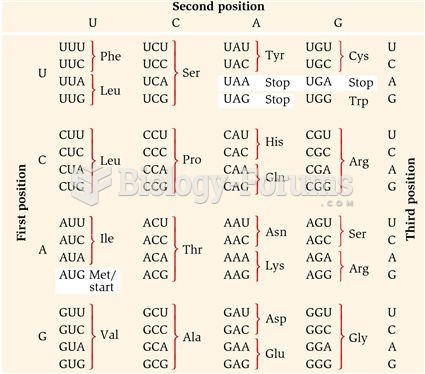 The Genetic Code
The Genetic Code
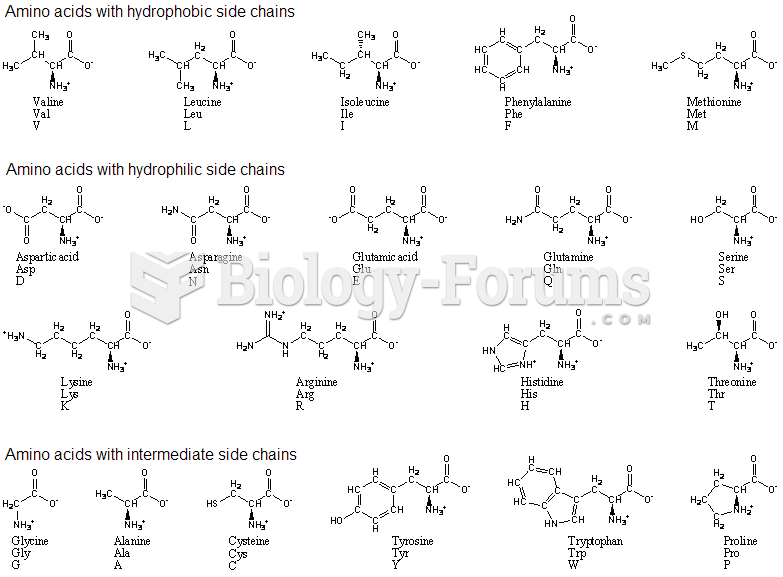 amino acids with single and three code
amino acids with single and three code
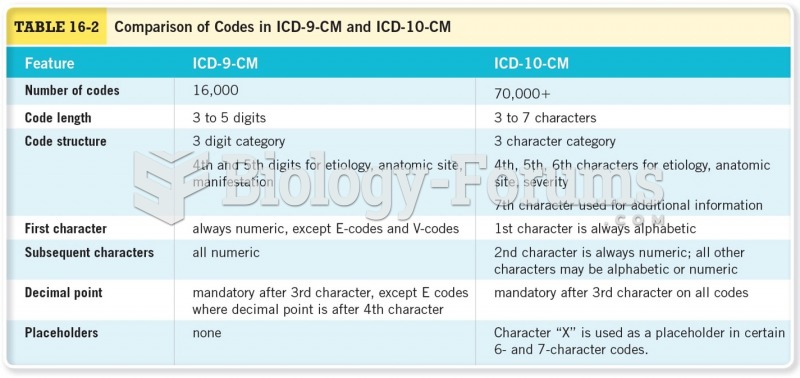 Comparison of Codes in ICD-9-CM and ICD-10-CM
Comparison of Codes in ICD-9-CM and ICD-10-CM
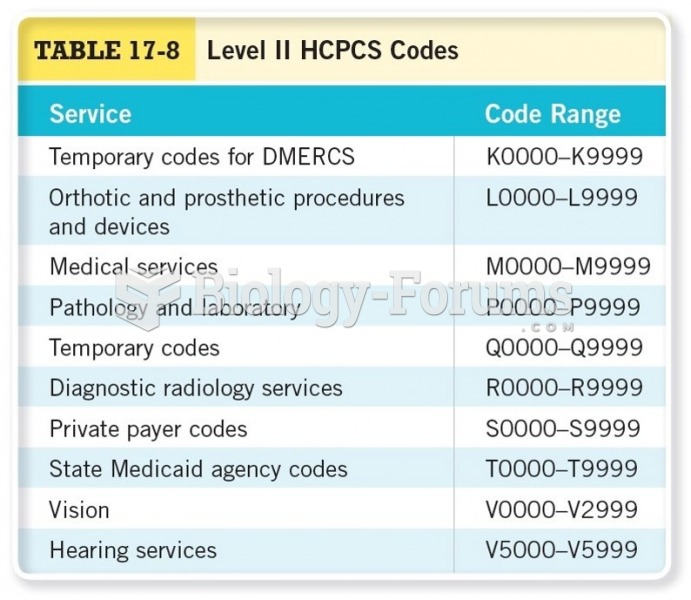 Level II HCPCs Codes Cont.
Level II HCPCs Codes Cont.
 Medical assistants who perform billing must know and use the proper codes to ensure third-party ...
Medical assistants who perform billing must know and use the proper codes to ensure third-party ...
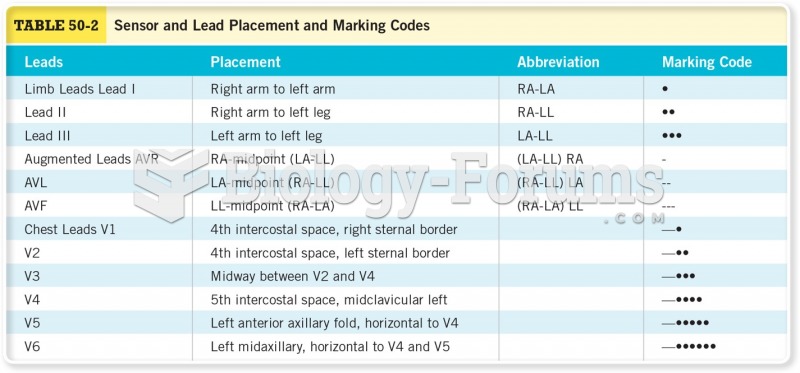 Sensor and Lead Placement and Marking Codes
Sensor and Lead Placement and Marking Codes