Code the following cases for inpatient facility purposes using ICD-9-CM and ICD-10-CM and PCS codes.
Calculate the MS-DRG.
Identify the Principal vs. Secondary diagnoses and procedures.
Use external cause codes when appropriate.
Do NOT code procedures that are captured by the facility chargemaster.
Secondary diagnoses and procedures do NOT need to be sequenced in any particular order.
Enter "None" when no code is required.
If more than one occurrence of a procedure is required, report the code with "x 2""x 3" etc.
INPATIENT HOSPITAL
Health Record Face SheetRecord Number: 70-50-77Age: 53Gender: Male Length of Stay: 2 DaysService Type: INPATIENT Discharge Status:
To HomeDiagnosis/Procedure: Idiopathic Dilated CardiomyopathyDISCHARGE SUMMARYPATIENT NAME: HUGH ACUTEADMISSION DATE: 06-23-XXDISCHARGE DATE: 06-25-XXDISCHARGE DIAGNOSIS:1. Idiopathic dilated cardiomyopathy, uncertain etiology.
2. Left bundle branch block.
3. Normal coronary arteries and normal hemodynamics.
PROCEDURES: Cardiac catheterization.
HISTORY OF PRESENT ILLNESS: The patient is a 53-year-old male admitted for evaluation of grossly abnormal Thallium test.
LABORATORY DATA: Glucose 106, BUN 11, creatinine 1.1, liver function tests are all normal, albumin 4.2, sodium 141, potassium 4.8, cholesterol 166, triglycerides 122, iron 82. White count 6900, hemoglobin 17.2, MCV 95, platelets 136,000.
Resting MUGA ejection fraction is performed. This shows an ejection fraction of 47%.
HOSPITAL COURSE: The patient is admitted to the hospital and taken to the cardiac catheterization lab. The patient's hemodynamics showed right atrial pressure 4, pulmonary artery 32/14, pulmonary capillary wedge is 6, cardiac output is 6.5, pulmonary vascular resistance is 186, and oximetry is unremarkable. Coronary arteries are all perfectly normal. There is no mitral regurgitation. Left ventricle is quite dilated. Ejection fraction angiographically is 46%. All walls are hypokinetic except for the anterobasilar wall, which is normal.
This is felt to be due to an idiopathic cardiomyopathy with normal hemodynamics.
A resting MUGA scan was obtained as a baseline. The patient was discussed with Dr. XYZ. The patient was discharged on 12/19 to be admitted on 12/19/xx to USA Hospital for myocardial biopsy.
DISCHARGE MEDICATIONS: Enteric aspirin 5 grains once a day and Capoten 12.5 mg 1½ tablets q 12 hours.
He is to follow up with me in a couple of weeks.
_____________________________
DR HEART, M.D.
HISTORY AND PHYSICALPATIENT NAME: HUGH ACUTEADMISSION DATE: 06-23-XXCHIEF COMPLAINT: Abnormal thallium treadmill. Admit for heart catheterization.
HISTORY OF PRESENT ILLNESS: The patient is a 38-year-old white male receiving primary care with a grossly abnormalthallium treadmill test. Admitted now for heart catheterization.
The patient really has minimal symptoms. He presented to the healthcare system recently for a complete physical just to make sure that everything was going fine. Dr. Know noted that the patient was having some fatigue and that he had a left bundle branch block. After discussing the case with Dr. Who, a thallium treadmill test was ordered which was quite abnormal as noted below.
ALLERGIES: None known.
MEDICATIONS: None.
SOCIAL HISTORY: The patient works in a potato cellar doing fairly manual labor. The patient smoked two packs of cigarettes daily for 30 years stopping 2 weeks ago. The patient is adopted and has no knowledge of his blood relatives.
MEDICAL HISTORY: He notes no exertional chest discomfort, neck discomfort, etc. of any type. He says that his exertional capacity and his exertional dyspnea is worse than it was 10 years ago, but feels that it is the same as it was 3 months ago and that it is the same as it was about a year ago. Apparently, he had an upper respiratory infection with productive cough, runny nose, sneezing, etc. this fall, but feels that he recovered satisfactorily from that. He does recall several episodes of epigastric discomfort manifest as a pressure sensation lasting perhaps a day at a time. He says he ignored it and it went away, and wondered whether he might have some gallbladder trouble. This never seemed to particularly get worse with exertion.
The patient has no orthopnea, PND, or edema. He has used two pillows on his bed at night under his head for a long time. He has occasional heart racing but no lightheaded spells, near syncope, or syncope. There is no history of hypertension, hyperlipidemia, diabetes, congenital heart disease, rheumatic fever, heart murmur, or MI.
REVIEW OF SYSTEMS: His general review of systems in detail is unremarkable. His only surgery is minor surgery on his knee. He does not use alcohol at all and never has. He uses one caffeinated beverage a day. He has no GI distress. He denies history of drug abuse, eye problems, cancer liver disease, emphysema, thyroid problems, gout, asthma, hay fever, hives, migraine headaches, TIA's, stroke, deep venous thrombosis, pulmonary embolism, kidney stones, etc.
PHYSICAL EXAMINATION:
GENERAL: BP 128/94, pulse 96, respirations distension.
LUNGS: Clear.
HEART: S1, S2 within normal limits with no murmurs, gallops, or rubs.
ABDOMEN: Unremarkable.
SKIN: Is warm and dry. Temp 97.9.
NECK: No jugular venous distension.
EXTREMITIES: There is no peripheral edema.
ELECTROCARDIOGRAM: Complete left bundle branch block, with frequent PVC's. Axis is +90°. Borderline right atrial enlargement.
EXERCISE THALLIUM TEST 06-21-XX
The patient exercised 5 minutes 37 seconds on a Bruce Protocol elevating his heart rate to 178 (107% predicted maximum), and blood pressure to 174/84. He was stopped because of fatigue. The patient's heart rate increased rapidly with exercise and at the end of 3 minutes of exercise, his heart rate was already 165. At the end of 2 minutes off exercise, it was 157. He remained in left bundle branch block throughout and there- were no significant ST changes and no arrhythmias. He had no chest discomfort. The images showed a dilated left ventricle with hypoperfusion of the anterior wall, septal wall, and posterior wall. There was some redistribution of the anterior and anteraseptal aspects of the heart. There was no redistribution of the inferior aspect.
ECHOCARDIOGRAM:
06-21-XX is technically limited, but shows severely reduced left ventricular function with normal chamber dimensions. Left atrium is at 3.9cm E point to septal separation is 1.4.
ASSESSMENT:1. High risk thallium scan with reduced IV function on echocardiogram inpatient with left bundle branch block and no symptoms.
2. Unknown family history.
3. Heavy smoking history.
PLAN: Admit for heart cath.
_________________________
DR. HEART, M.D.
CARDIAC CATHETERIZATION LABORATORYPATIENT NAME: HUGH ACUTEPROCEDURE REPORT:PROCEDURE: Right and left heart catheterization, selective coronary angiography and left ventriculography.
PROCEDURE NOTE: The patient is brought to the cardiac catheterization lab, and the right inguinal area is prepped and draped in the usual manner. Using Seldinger technique, both the right femoral artery and right femoral vein are cannulated, and sheath introducers are placed in each vessel. All catheter manipulations are done using a guidewire and under fluoroscopic control. A fiberoptic Swan-Ganz catheter is positioned in the right heart. A pigtail catheter is positioned in the ascending aorta. Hemodynamic pressure measurements are-made. The aortic valve is crossed in a retrograde manner. Hemodynamic pressure measurements are made. Thermodilution cardiac output is measured. Oximetry is measured in the right and left heart. The Swan-Ganz catheter is removed.
Left ventriculography is performed in the RAO projection and is recorded on 35 mm cineangiographic film. The catheter is then pulled back across the aortic valve while pressure measurements are being made.
The catheter is then exchanged over a guidewire for a Judkin's left coronary catheter, and left coronary cineangiography is performed in multiple projections in the usual manner. The catheter is then exchanged over a guidewire for a Judkins right catheter, and right coronary cineangiography is performed in the usual manner.
At the conclusion of the case, hemostasis is obtained after catheters were pulled. There are no complications.
HEMODYNAMIC FINDINGS: Right atrial pressure mean is 4 mm. of mercury. X and Y descent appear to be normal. The right ventricular end diastolic pressure is equal to the left ventricular end diastolic pressure. These two pressure waveforms are superimposed throughout diastole. Pulmonary artery pressure is 32/14, mean 21. Pulmonary capillary wedge mean is 6, with a normal V wave. Left ventricular pressure is 125/, 8. Aortic pressure is 125/65, mean 86. There is no gradient across the mitral valve during diastole or across the aortic valve during systole. Thermodilution cardiac output is 6.46 liters per minute. Systemic vascular resistance is 1015. Pulmonary vascular resistance is 186. Oximetry on blood samples shows saturation as follows: pulmonary artery 65%, right ventricle 64%, right atrium 64.7%, vena cavae 65%. Room air blood gas in the left ventricle 7.45, P02 62, PCO2 37, Bicarb. 26, Saturation 89%.
LEFT VENTRICULOGRAM: There no mitral regurgitation. The anterobasilar wall moves normal. All other walls of the ventricle are hypokinetic. The left ventricle is moderately dilated, with an end diastolic volume of 321 cc's (upper limits of normal for his body surface area is 257 cc's). Ejection fraction is measured on several beats and ranges between 42 and 52%.
CORONARY ANGIOGRAPHY: The coronary arteries are perfectly smooth and within normal limits. The LAD gives rise to a moderate sized first diagonal branch and a moderately large second diagonal branch. There is a large bifurcated ramus intermedius branch. There are two moderately large posterolateral branches of the circumflex. The right coronary artery gives rise to the posterior descending artery and one posterolateral branch.
CONCLUSIONS:
1. Normal coronary arteries.
2. Dilated hypocontractile left ventricle with no mitral regurgitation.
3. Normal hemodynamics and cardiac output.
4. Normal oximetry.
5. Mild resting hypoxia.
This picture is consistent with an idiopathic dilated cardiomyopathy.
______________________________
DR. HEART, M.D.
ICD-9-CM diagnosis code(s): PDx_____________________
SDx _____________________
ICD-9-CM procedure code(s): PPx_____________________
SPx_____________________
ICD-10-CM diagnosis code(s): PDx_____________________
SDx _____________________
ICD-10-PCS procedure code(s): PPx_____________________
SPx_____________________
MS-DRG: _____________________

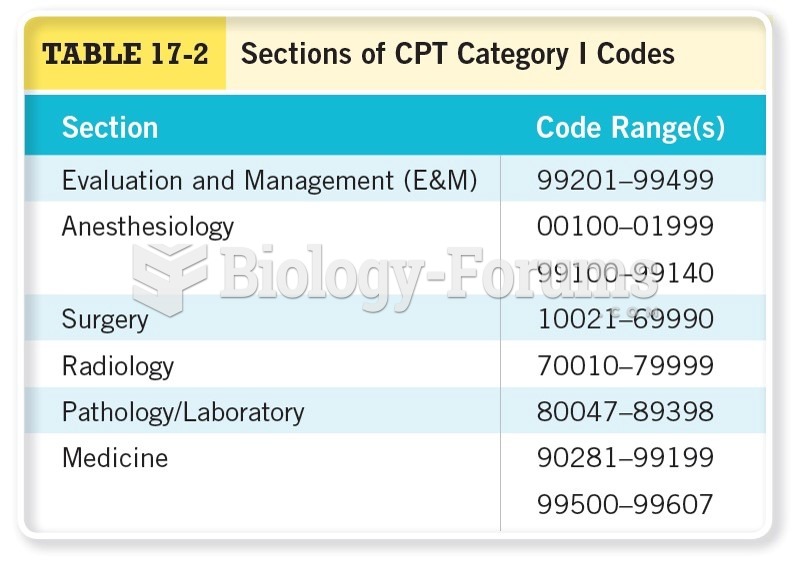 Sections of CPT Category I Codes
Sections of CPT Category I Codes
 Review Bundling, Add-on Codes, and Quantity Edits
Review Bundling, Add-on Codes, and Quantity Edits
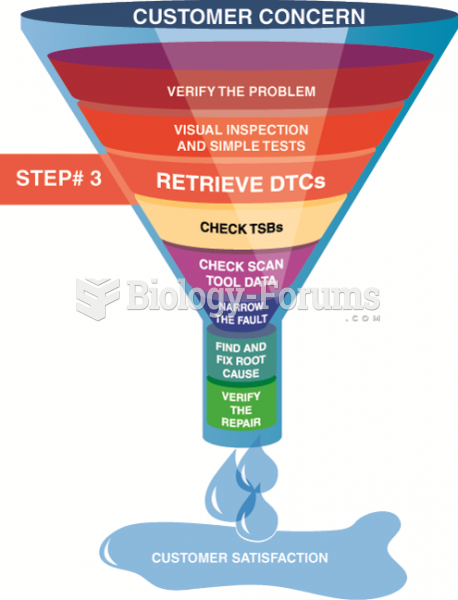 Step 3 in the diagnostic process is to retrieve any stored diagnostic trouble codes.
Step 3 in the diagnostic process is to retrieve any stored diagnostic trouble codes.
 After checking for stored diagnostic trouble codes (DTCs), the wise technician checks service ...
After checking for stored diagnostic trouble codes (DTCs), the wise technician checks service ...
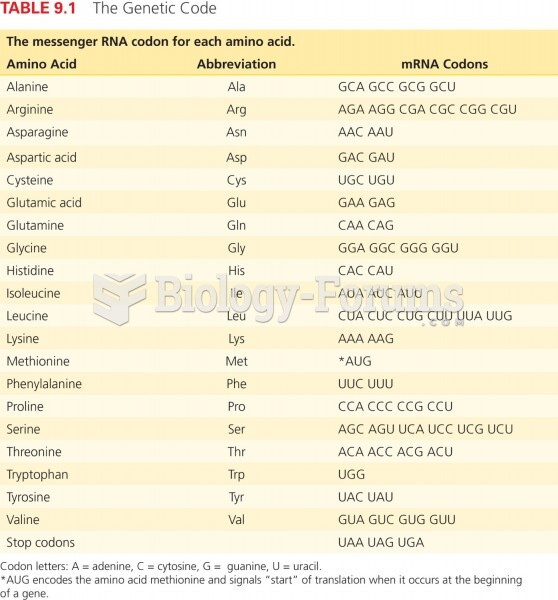 The Genetic Code
The Genetic Code
 A manufacturer of cat towers wishes to locate a super assembly facility to meet their cat tower ...
A manufacturer of cat towers wishes to locate a super assembly facility to meet their cat tower ...