This topic contains a solution. Click here to go to the answer
|
|
|

 The grey nurse shark is critically endangered on the Australian east coast.
The grey nurse shark is critically endangered on the Australian east coast.
 The nurse needs to inform the patient with impaired vision when a touch is to occur and ask permissi
The nurse needs to inform the patient with impaired vision when a touch is to occur and ask permissi
 Assessing for McMurray's Sign
Assessing for McMurray's Sign
 A physician is performing a colonoscopy on a client and viewing the internal structures of the colon
A physician is performing a colonoscopy on a client and viewing the internal structures of the colon
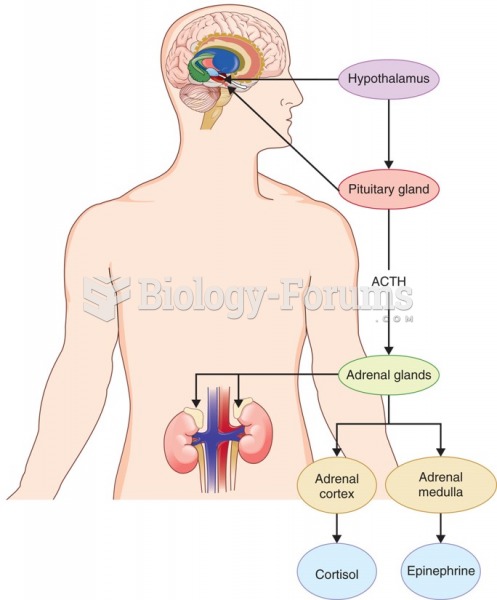 According to neuroendocrine models of depression, repeated or chronic stress results in overactivity ...
According to neuroendocrine models of depression, repeated or chronic stress results in overactivity ...
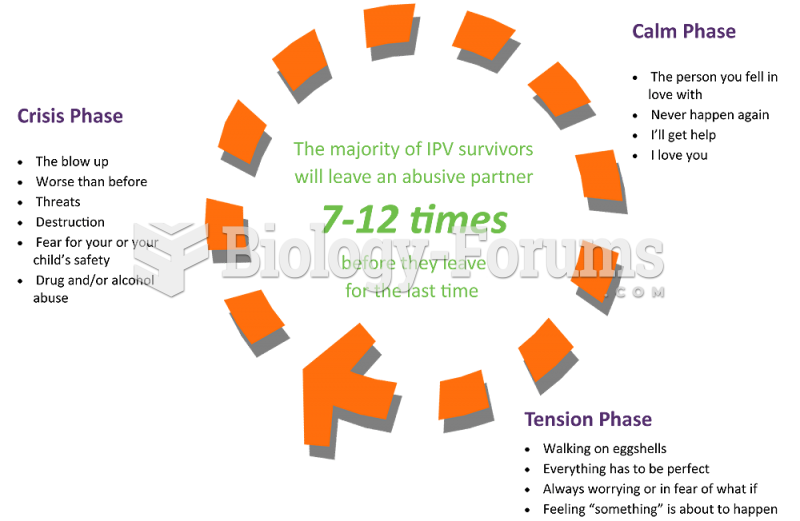 A patient is talking to the nurse about her husband’s abuse and attempt to strangle her. She ...
A patient is talking to the nurse about her husband’s abuse and attempt to strangle her. She ...