This topic contains a solution. Click here to go to the answer
|
|
|

 Rinne Test, Assessing Air Conduction
Rinne Test, Assessing Air Conduction
 C, A nurse can also administer the medication by setting the dose and rate with an electronic infusi
C, A nurse can also administer the medication by setting the dose and rate with an electronic infusi
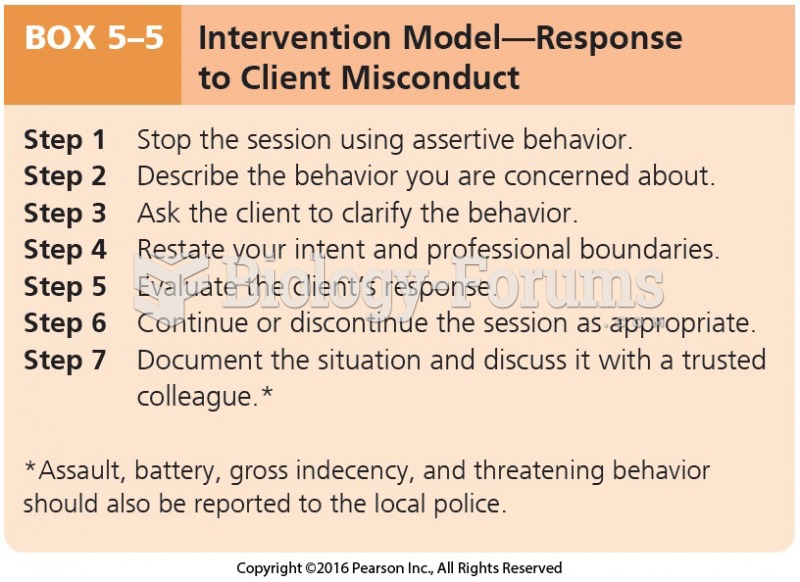 Intervention Model-Response to Client Misconduct
Intervention Model-Response to Client Misconduct
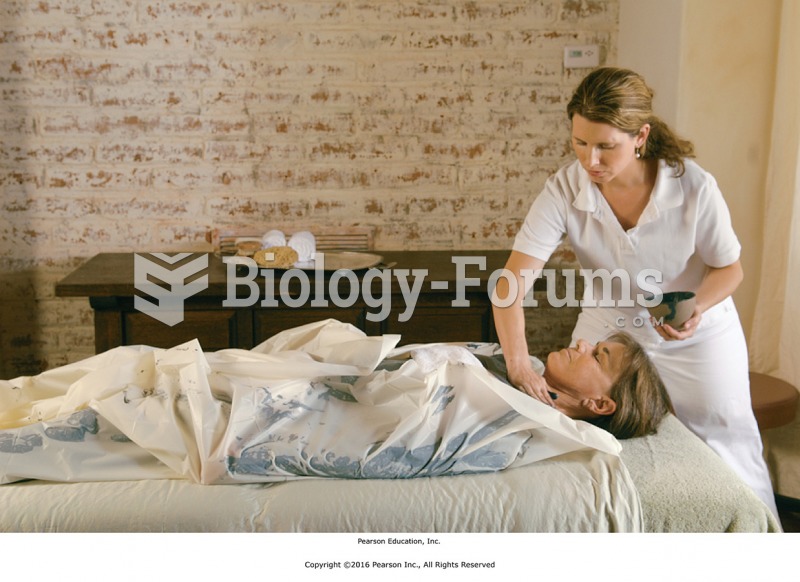 Apply the substance to the client’s upper chest.
Apply the substance to the client’s upper chest.
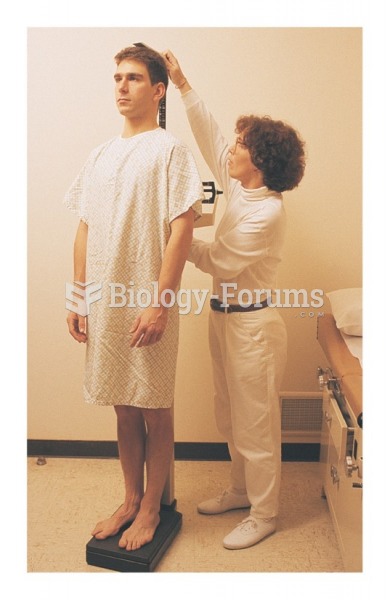 Measuring the client’s height with a platform scale
Measuring the client’s height with a platform scale
 depression
depression