Answer to Question 1
Figures 1-2 and 1-3 compare the workflow of offices using paper and electronic charts in 12 steps. Students should identify most of the differences.
Any acceptable comparison of those figures should suffice. Here is a summary of key differences:
Both workflows started with the patient calling for an appointment.
Astute students may point out that an alternative for some EHR offices is to allow scheduling over the Internet; extra points for those students.
Paper: Paper charts are pulled the night before the visit.
EHR: Pulling charts is not necessary; however, some EHR systems can automatically verify the patient's insurance eligibility.
Paper: The patient updates his or her history on a paper form.
EHR: The patient completes his or her medical history and reason for the visit using a computer in a private area of the waiting room.
Paper: The patient describes symptoms and reason for the visit to the nurse; vital signs are recorded in the paper chart by the nurse. The doctor enters, and the patient repeats the description of symptoms and reason for the visit.
EHR: The nurse reviews patient -entered data with the patient and edits for clarification if necessary. Vital signs can be electronically transferred from instruments into chart.
The clinician performs the physical exam and makes a clinical assessment and a plan of treatment.
Paper: The clinician makes a few notes and retains the observations and physical exam in his or her memory.
EHR: The clinician records the findings at the time of the exam or shortly thereafter; has access to previous problems and reviews those; and makes the clinical assessment and plan of treatment.
Paper: The clinician hand writes prescriptions and orders, makes a note of them in the paper chart, and marks billing codes and diagnosis codes on the paper encounter form. The clinician creates the exam note from memory, either hand writing in the chart or dictating.
EHR: The clinician enters the findings directly into the EHR while the patient is present. Orders create tasks for lab personnel to obtain a specimen, which is subsequently transmitted directly to the lab.
Prescriptions are written as part of the chart and transmitted to the pharmacy.
Paper: Dictated notes must be transcribed and subsequently reviewed and signed by the clinician and then filed in the paper chart.
EHR: When the exam is finished, the note is finished. A copy of the completed note can be printed and given to the patient with other patient education materials.
The patient checks out.
Paper: Billing information is manually keyed into the computer from the encounter form. The codes circled by the clinician are only a best guess and may require a coding specialist to verify them.
EHR: The billing codes can be automatically calculated from the completed note and electronically transferred from the EHR into the billing system.
Paper: Results from tests are returned, and the chart is pulled again.
The doctor must review and sign the result s, staff must notify the patient, and the chart must be refiled.
EHR: Results received electronically are merged directly into the patient chart and immediately available for clinician review and patient notification.
Answer to Question 2
The patient checks in with the receptionist.
In the waiting area, the patient updates his or her medical historyand reason for the visit.
The patient moves to an exam room, and a nurse takes vitals and reviews the symptoms and reason for visit.
The physician enters, reviews the chart, and discusses the symptoms and reason for the visit. If it is necessary for patient to disrobe, the doctor usually leaves to see another patient, then returns to perform the clinical exam.
The clinician performs a physical exam, accesses patient condition, writes orders for tests or prescriptions, provides education or counseling, and dictates or updates the chart.
If tests have been ordered, a specimen is taken or the patient is given directions to an outside lab.
The patient is given educational material and prescriptions and checks out.

 Indian paper wasp (Ropalidia) colony with eggs
Indian paper wasp (Ropalidia) colony with eggs
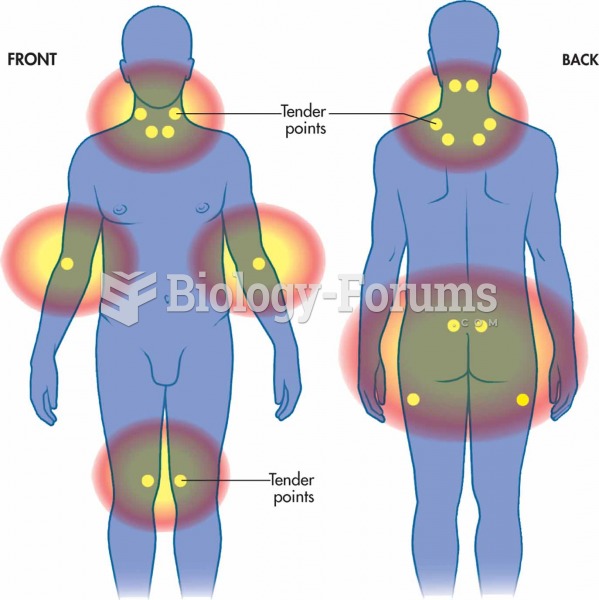 The 18 tender points of fibromyalgia
The 18 tender points of fibromyalgia
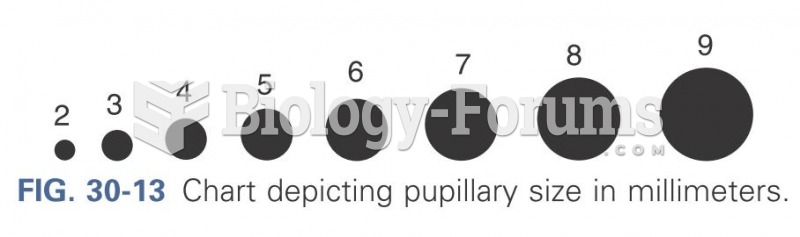 Chart depicting pupillary size in millimeters
Chart depicting pupillary size in millimeters
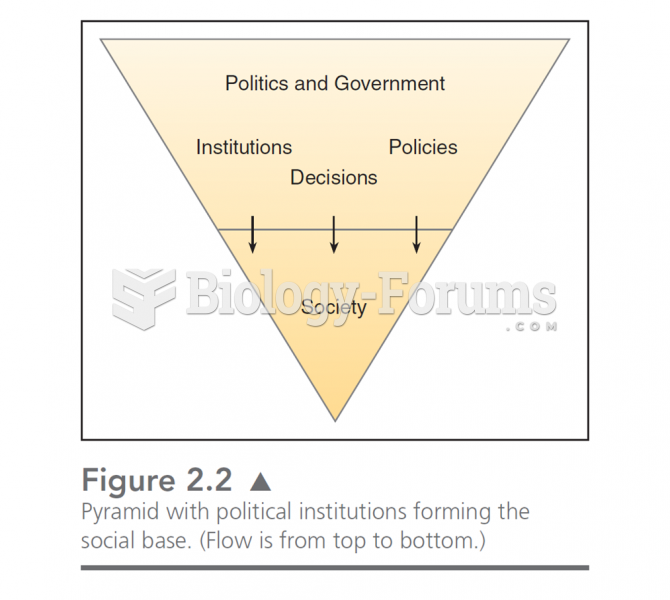 This chart illustrates the “drip down” model of government. In this, politics is formed by the soc
This chart illustrates the “drip down” model of government. In this, politics is formed by the soc
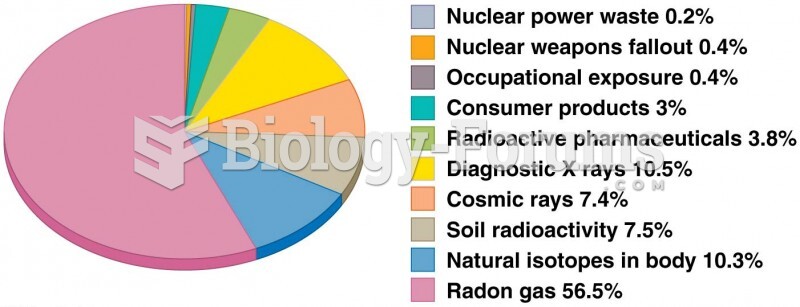 Chart showing average yearly dose of radiation from natural and human-made sources
Chart showing average yearly dose of radiation from natural and human-made sources
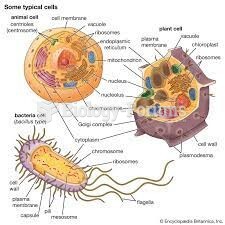 IMAGES THAT DESCRIBE CELLULAR PARTS
IMAGES THAT DESCRIBE CELLULAR PARTS