The nurse assessing a client with depression could use which of the following to help with the assessment process?
1. Glasgow Coma Scale
2. Beck Depression Inventory
3. The client's family members, for answering the assessment questions
4. More time talking with the client
Question 2
An 82-year-old man is admitted to a medicalsurgical unit for diagnostic confirmation and management of probable delirium.
After assessment by the team caring for the client, which of the following statements by the client's daughter most supports the team diagnosis? 1. Maybe it's just caused by aging. This usually happens by age 82..
2. The changes in his behavior came on so quickly. I wasn't sure what was happening.
3. Dad just didn't seem to know what he was doing. He would forget what he had for breakfast..
4. Dad has always been so independent. He's lived alone for years since my mom died..

 The postoperative client supports an incision with a folded pillow when taking a deep breath and cou
The postoperative client supports an incision with a folded pillow when taking a deep breath and cou
 Nurse Sandy
Nurse Sandy
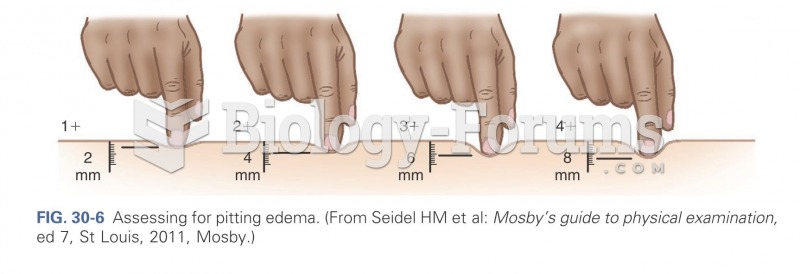 Assessing for pit edema
Assessing for pit edema
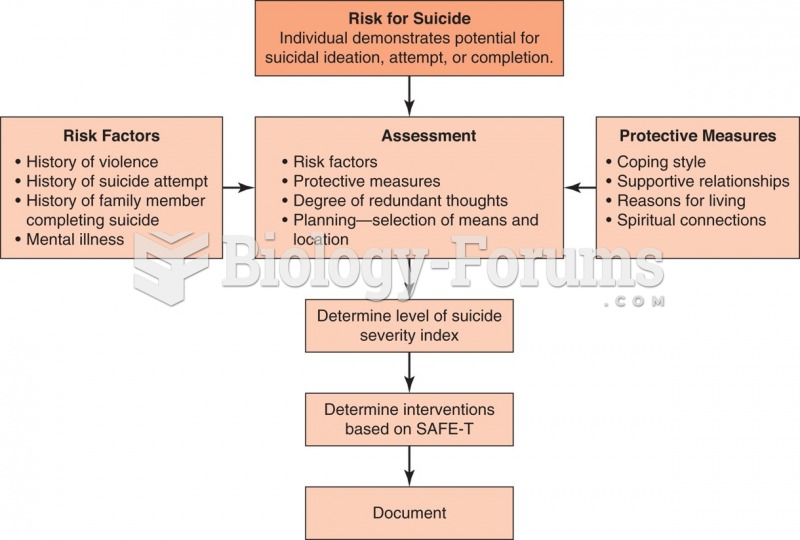 Algorithm for assessing a patient at risk for suicide.
Algorithm for assessing a patient at risk for suicide.
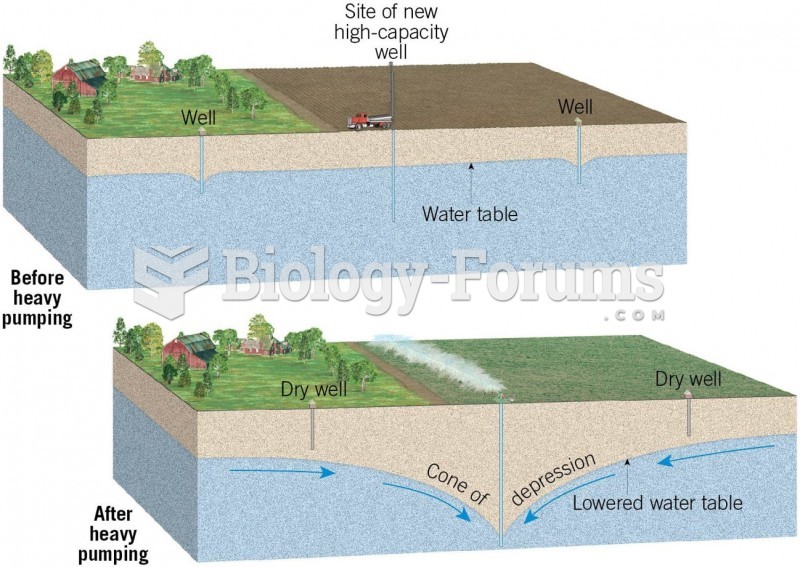 Cone of Depression Formation
Cone of Depression Formation