Answer to Question 1
Answer:
Iron-deficiency anemia: decreased; the etiology of IDA is such that when a patient's iron need exceeds intake, the body utilizes its iron stores and decreases them; is often one of the first signs of iron-deficiency anemia
Anemia of chronic disease: adequate to increased; the problem is impaired ferrokinetics. There is adequate intake of iron but poor utilization of it. The primary protein abnormality that is responsible for this abnormal utilization is hepcidin. Hepcidin is produced in response to inflammatory cytokines, which are increased in patients with ACD, so the disorder often arises from an exacerbated inflammatory response.
Thalassemia: adequate to increased; the defect is improper globin chain synthesis, not iron usage.
Sideroblastic anemia: increased; this is the opposite of IDA. Iron intake exceeds the body's need for iron and can be improperly utilized.
Answer to Question 2
Answer:
Flow cytometry: malignant lymphomas and leukemias; evaluates for minimal residual disease after chemotherapy
Cytogenetics: acute leukemias, malignant lymphomas, MDS, and MPDs; helps determine diagnosis and prognosis. Also can detect relapse.
Molecular genetics: hematolymphoid malignancies; can detect minimal residual disease
Cytochemical staining: subsets of acute leukemia; differential diagnosis of acute and chronic leukemias, such as ALL, AML, CML, CLL, and HCL.

 blue bird of paradise
blue bird of paradise
 workbook pages answers
workbook pages answers
 Performing a Gram Stain
Performing a Gram Stain
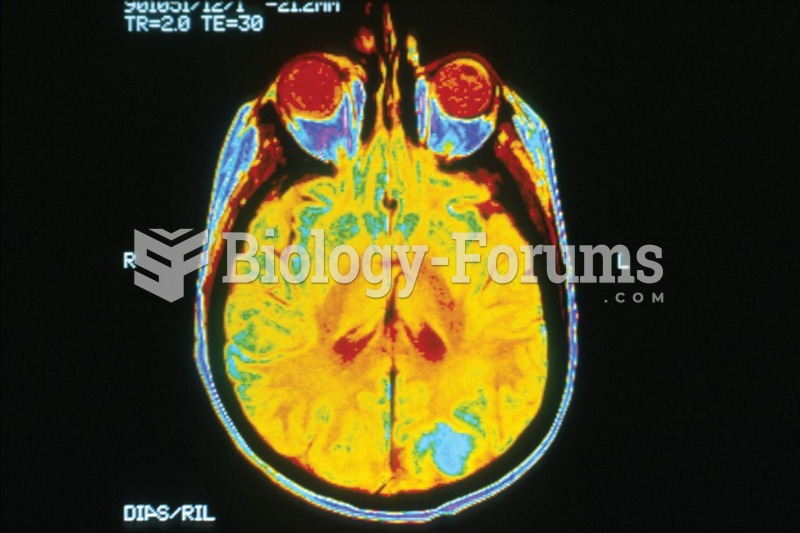 MRI image of brain cancer. The bright blue color indicates where the cancer has metastasized.
MRI image of brain cancer. The bright blue color indicates where the cancer has metastasized.
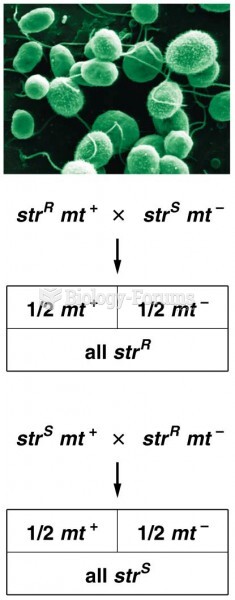 The results of reciprocal crosses between streptomycin-resistant and streptomycin-sensitive
The results of reciprocal crosses between streptomycin-resistant and streptomycin-sensitive
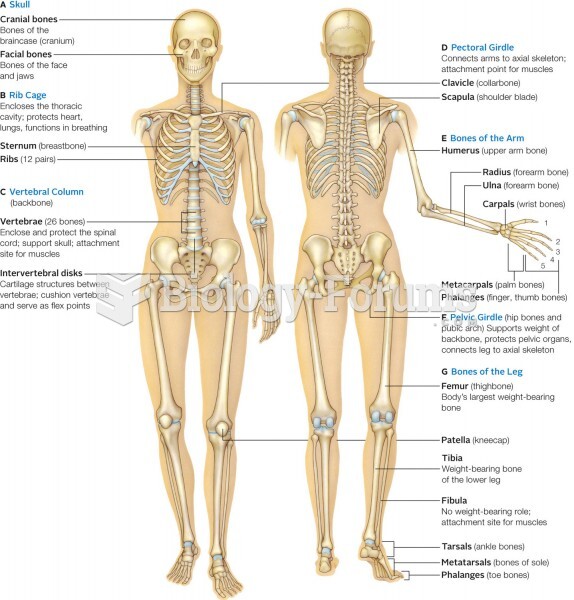 Major bone (tan) and cartilage (light blue) elements of the human skeleton. Inset shows regions of v
Major bone (tan) and cartilage (light blue) elements of the human skeleton. Inset shows regions of v