Answer to Question 1
Correct Answer: 3
Clients experiencing tremendous loss often develop depression as part of their reaction to grief. However, this depression should also be seen with other stages of the grieving process such as denial, anger, bargaining, and acceptance. Clients remaining in one stage of the grieving process may not be progressing toward acceptance. There are not enough data to support the remaining nursing diagnoses. Powerlessness refers to feelings of a loss of control with the situation. Anxiety infers feelings of apprehension. Spiritual distress infers the client would be at odds with her feelings.
Answer to Question 2
Correct Answer: 2
Evaluation is the process whereby the progress toward achieving the goals is reviewed and documented. Implementation is the process of performing certain interventions designed to move the client toward achievement of the goal. During the planning phase of the nursing process, nursing diagnoses are formulated after data have been assessed, and then goal setting takes place. Assessment is the process by which data are collected.

 A nurse shows empathy to a client.
A nurse shows empathy to a client.
 Older adults may grieve intensely over the loss of a person or situation that has been a part of the
Older adults may grieve intensely over the loss of a person or situation that has been a part of the
 Mass Loss by a Supermassive Star
Mass Loss by a Supermassive Star
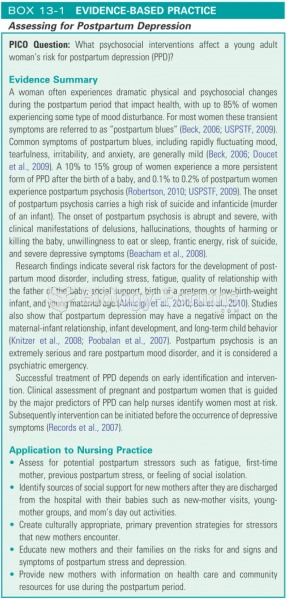 Assessing for postpartum depression
Assessing for postpartum depression
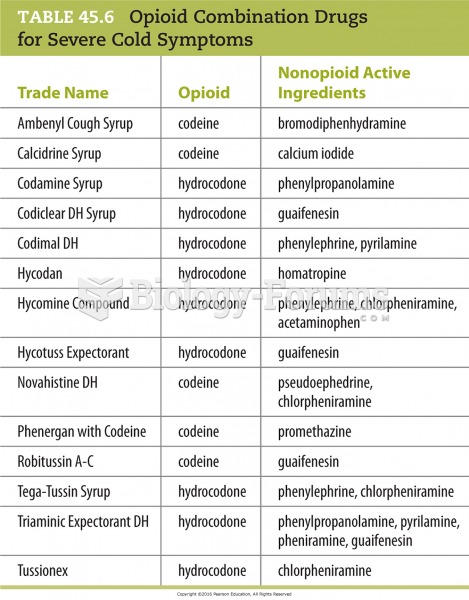 Opioid Combination Drugs for Severe Cold Symptoms
Opioid Combination Drugs for Severe Cold Symptoms
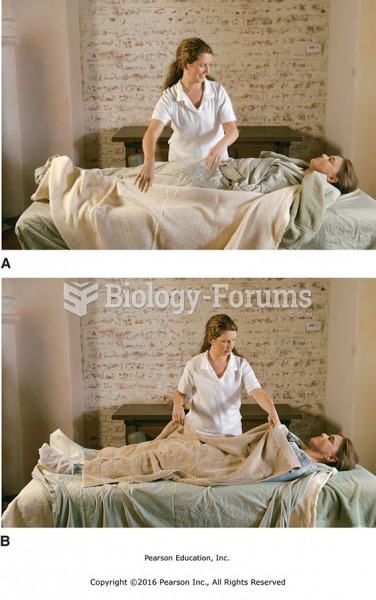 (A) Unwrap each of the layers until the client is covered by just the plastic sheet and the towels ...
(A) Unwrap each of the layers until the client is covered by just the plastic sheet and the towels ...