This topic contains a solution. Click here to go to the answer
|
|
|

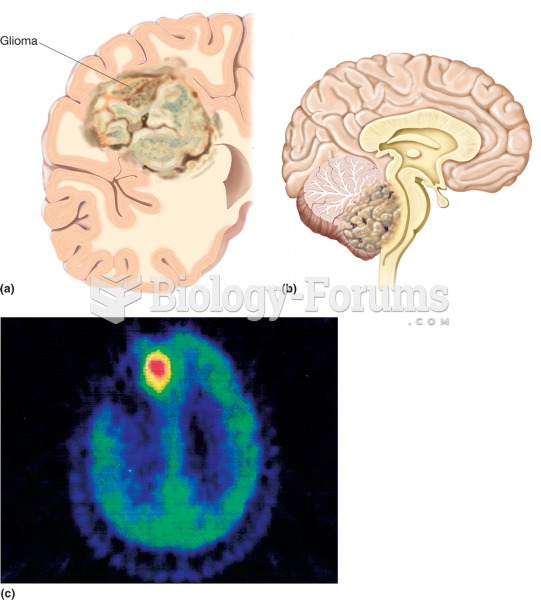 Glioma. (a) Illustration of a large glioma (colored area) within the left cerebral hemisphere in a s
Glioma. (a) Illustration of a large glioma (colored area) within the left cerebral hemisphere in a s
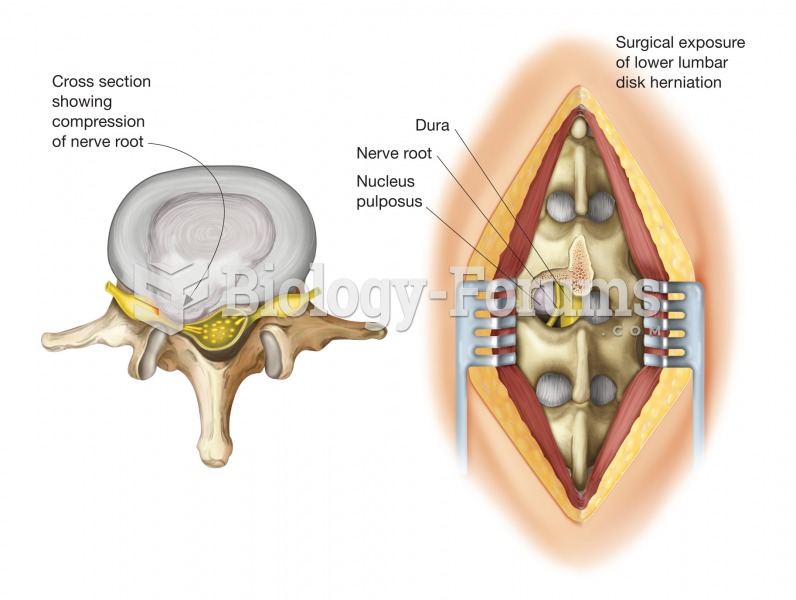 Herniated disk. A herniated disk is a protrusion of the disk’s gelatinous center, called the nucleus
Herniated disk. A herniated disk is a protrusion of the disk’s gelatinous center, called the nucleus
 To check pupillary reflexes the nurse first holds the penlight
To check pupillary reflexes the nurse first holds the penlight
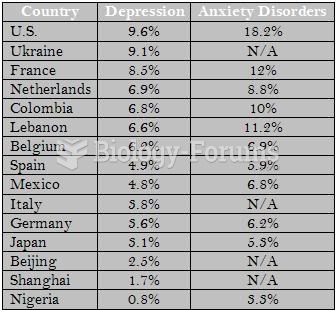 Depression
Depression
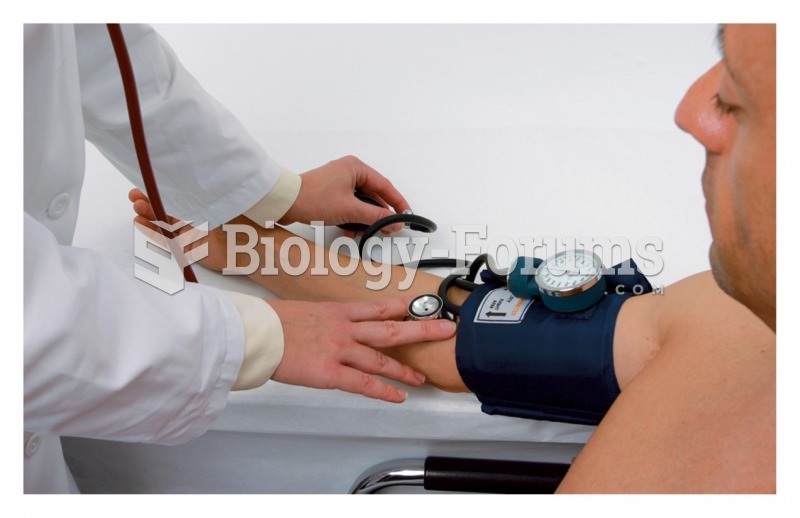 Measuring the client’s blood pressure
Measuring the client’s blood pressure
 Mechanisms involved in production of metabolic alkalosis due to loss of gastric fluid
Mechanisms involved in production of metabolic alkalosis due to loss of gastric fluid