Answer to Question 1
Some definitions of public health stress that public health involves the health of the whole community, even the whole world, not just the medical treatment of individuals. Because social inequality and absolute poverty are important determinants of health, the field of public health goes far beyond the scope of this text. That is, a poor country with a more equal distribution of wealth and income may have a healthier population than a rich country with an unequal distribution of wealth. For example, the United States, which is ranked first in health spending, has a health system that is ranked 37th in the world by the World Health Organization (WHO), which is the directing and coordinating authority for health within the United Nations system. In terms of longevity and infant mortality, statistics show that the United States is not among the top 20 nations in the world. Therefore, to effectively address questions on the health of a local community, a nation, or the international community, one has to minimize or at least decrease social inequalityfor example, by providing universal health care, day care, and subsidies to bring people above the poverty line or by using the tax system to reduce inequality (rather than redistributing income to the top, as we have been doing).
In the United States, economic and social inequalities have been increasing since 1967 . This means that the distribution of income and wealth has been increasingly unequal and that the opportunity for social mobility has decreased.
The fact that health depends more on social class and relative inequality than on the availability of medical treatment was recognized in 1975 by Theodore Cooper, then U.S. Assistant Secretary for Health: It is one of the great and sobering truths of our profession that modern health care probably has less impact on the population than economic status, education, housing, nutrition and sanitation. Yet we have fostered the idea that abundant, readily available high quality health care would be some kind of panacea for the ills of society and the individual. This is a fiction, a hoax. It has been hypothesized that the constant stress on poor people in a highly stratified society may account for higher rates of illness and death. These questions are beyond the scope of this text, but they need to be mentioned in any honest discussion of public health.
According to data from the Congressional Budget Office, inequality in the United States continues to grow. Between 1979 and 2007, the income gap between the top 1 percent and the middle and poorest fifths of the population tripled. In 2007, the share of after-tax income going to the top 1 hit its highest level (17.1 percent) since 1979, while the share going to the middle fifth of Americans shrank to its lowest level during this period (14.1 percent). Adjusted for inflation, during the same period, after-tax incomes for the top 1 percent rose by 281 percent (about a 973,100 increase per household) compared to 25 percent (11,200) for the middle fifth and 16 percent (2400) for the bottom fifth. The average household at the top had an income of 1.3 million (up 88,000 in one year). The average middle income household earned 55,300, and the average bottom fifth income was
17,700.
The gap between the top 1 percent and the poorest fifth grew from 22.7 times higher in 1979 to 74.6 times higher, more than tripling the income gap in less than 30 years. The average after-tax income of the top 1 percent nearly quadrupled, while that of the bottom fifth grew by only 16 percent. The incomes at the very top (in the 99.99th percentile) have soared from about 2 million in the 1970s to about 10 million in 2009.
As the incomes at the top continue to grow, the number of people in poverty and the percentage of the population in poverty also continue to grow. According to the Census Bureau, in 2008, there were 39.8 million people in poverty (13.2 percent); in 2009, however, 43.6 million people (14.3 percent) were living below the poverty line (21,954 for a family of four). Statistics on poverty have been kept for 51 years. In 2009, more people were poor than in any previous year for which data are available.
In 2011, the U.S Centers for Disease Control and Prevention (CDC) published a report on health disparities and inequality. A health disparity is a particular type of health difference that is closely linked with social, economic, and/or environmental disadvantage, according to Department of Health and Human Services. The CDC found that the data pertaining to inequalities in income, morbidity, mortality, and self-reported healthy days highlight the considerable and persistent gaps between the healthiest persons and states and the least healthy. The CDC also found that the correlation between poor health andinequality at the state level holds at all levels of income. In addition, inequality existed in infant mortality between African Americans and whites and in death from stroke and heart disease between African Americans and whites. Minorities are less likely to get preventive care and, when sick, less likely to receive quality health care. As incomes get lower, rates of preventable hospitalizations rise.
Answer to Question 2
D

 These school-age childrean are eating a health snack
These school-age childrean are eating a health snack
 Relationship of the electrocardiogram to electrical conduction in the heart.
Relationship of the electrocardiogram to electrical conduction in the heart.
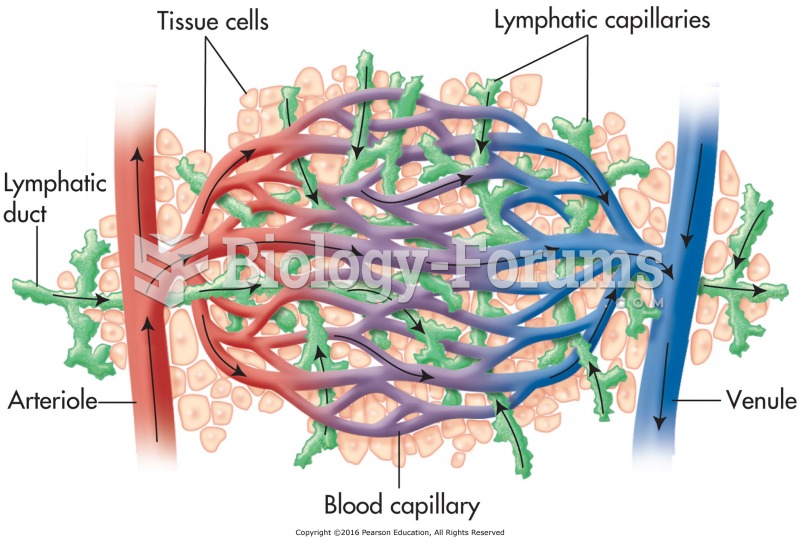 Relationship of the lymphatic system to the cardiovascular system.
Relationship of the lymphatic system to the cardiovascular system.
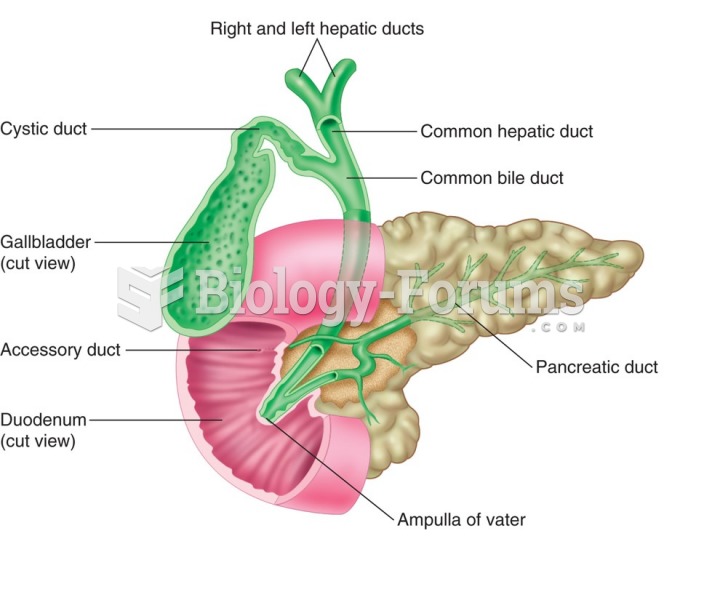 Relationship between the pancreas and the digestive system.
Relationship between the pancreas and the digestive system.
 The Importance of Social Connection
The Importance of Social Connection
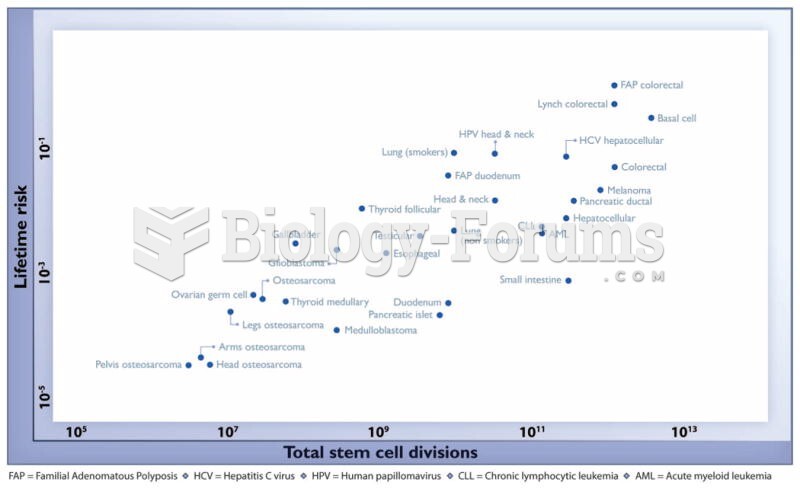 The relationship between the number of stem cell divisions in the lifetime of a given tissue and the
The relationship between the number of stem cell divisions in the lifetime of a given tissue and the