Answer to Question 1
Correct Answer: 1,3
Rationale 1: The dentist should be made aware that the client takes aspirin daily.
Rationale 2: Doses as small as 75 mg/day can increase the risk of bleeding.
Rationale 3: The usual recommendation is to discontinue use of aspirin a week prior to any dental or surgical procedure.
Rationale 4: Aspirin therapy can cause bleeding from dental procedures.
Rationale 5: Vitamin E does not reverse bleeding.
Global Rationale: The antiplatelet effects of aspirin can promote bleeding at sites other than the GI tract even in doses as small as 75 mg/day. Because it irreversibly inhibits COX-1 in platelets, the antiplatelet action of aspirin can be prolonged. It may take longer for minor cuts and injuries to stop bleeding. Patients undergoing surgical or dental procedures should discontinue aspirin use a week prior to the procedure. Vitamin E does not reverse bleeding.
Answer to Question 2
Correct Answer: 1,2,4
Rationale 1: The risk of gastrointestinal bleeding is greater in people over age 60.
Rationale 2: The risk of gastrointestinal bleeding is greater in people who smoke.
Rationale 3: Taking vitamin C is neither a recommendation nor a contraindication for use of aspirin.
Rationale 4: Clients with gastric ulcer disease have a higher risk of gastrointestinal bleeding while taking aspirin.
Rationale 5: Being of Hispanic heritage has no impact on whether aspirin therapy is safe.
Global Rationale: The most significant adverse effect of aspirin and other NSAIDs is GI bleeding. Although the risk is dose related, even low doses of aspirin (75325 mg/day) may double the risk of GI bleeding. Risk factors for aspirin-induced GI bleeding include history of peptic ulcers, age greater than 60, use of anticoagulants or corticosteroids, Helicobacter pylori infection, smoking, and use of alcohol. Use of vitamin C and being of Hispanic heritage are not significant determinants in the use of NSAIDs.

 The nurse is using Standard Precautions to draw blood.
The nurse is using Standard Precautions to draw blood.
 The nurse assesses the patient's ability to use the walker correctly
The nurse assesses the patient's ability to use the walker correctly
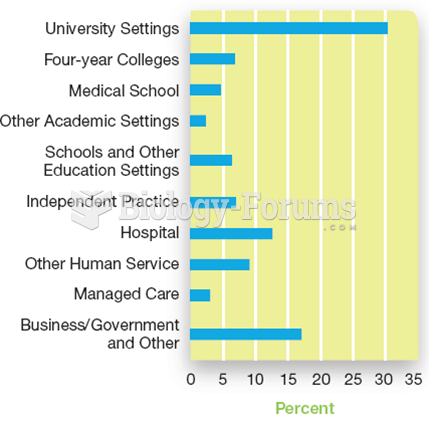 Where Professional Psychologists Work Primary employment settings for PhD recipients in psychology.
Where Professional Psychologists Work Primary employment settings for PhD recipients in psychology.
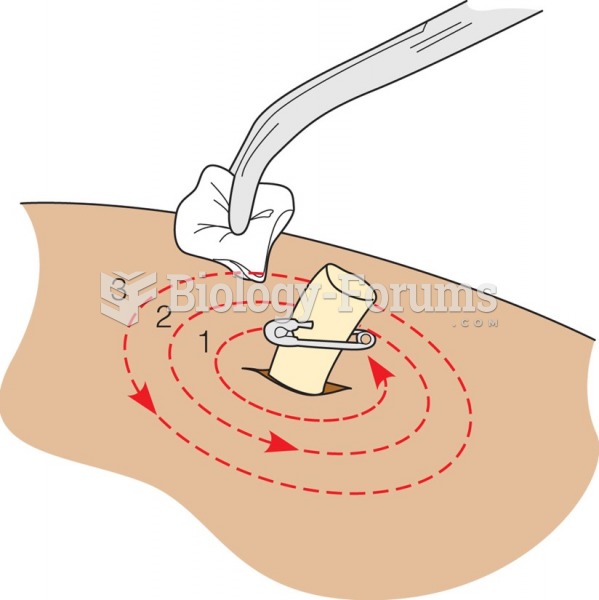 To cleanse an open wound, begin close to the wound and work outward in full or half circles.
To cleanse an open wound, begin close to the wound and work outward in full or half circles.
 Work and Gender: Women at Work in India
Work and Gender: Women at Work in India
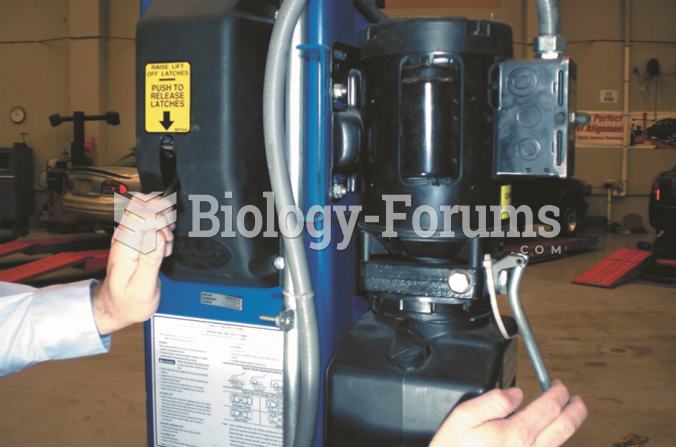 When the service work is completed, the hoist should be raised slightly and the safety released ...
When the service work is completed, the hoist should be raised slightly and the safety released ...