Answer to Question 1
Hyperglycemia has been shown to correlate with poor outcomes in the ICU patient. It has been shown to lead to increased length of stay and higher risk of in-hospital mortality. Also, in patients with known DM before admission, it has been shown to increase the risk for infection and shock. For our patient, the hyperglycemia was treated using an insulin drip protocol, which is a commonly used therapy in critically ill patients. Tight blood glucose control (80-110 mg/dL) does not confer advantages in these patients. Both Society of Critical Care Medicine (SCCM) and ASPEN recommends a goal of 110 to 150 mg/dL while the American Diabetes Association (ADA) and the American Association of Clinical Endocrinologists recommends a goal of 140-180 mg/dL as a reasonable goal for these patients.
Answer to Question 2
When a patient is receiving nutrition support, it is important to monitor: physical assessment (signs of fluid and nutrient excess or deficiency), functional status (mobility, sedation), vital signs, actual nutrient intake (oral, enteral, and parenteral) in comparison to nutrition prescription, weight and weight changes, pertinent labs (blood glucose, triglycerides, inflammatory markers, BUN, liver function enzymes, electrolytes), medications administered (propofol, SSI), and changes in gastrointestinal function (bowel sounds, I/O, stool output). Additionally, the RD should ensure that the head of bed is at a 30o-45o angle (for EN) and tube patency is maintained.
Monitor wound healing and the progress of his open abdominal wound closure. This can confirm (or not) the adequacy of the patient's nutrient intake. Nitrogen balance can be helpful to measure the adequacy of nutrient intake as well, even though this can be altered with the abdominal wounds and metabolic stress.

 (a) Feeding by bear on salmon results in large allochthonous inputs of nutrients into (b) the forest
(a) Feeding by bear on salmon results in large allochthonous inputs of nutrients into (b) the forest
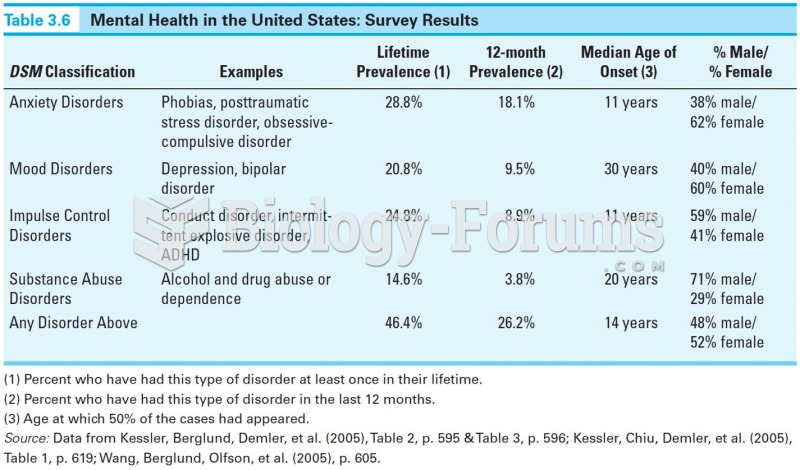 Mental Health in the U.S: Survery Results
Mental Health in the U.S: Survery Results
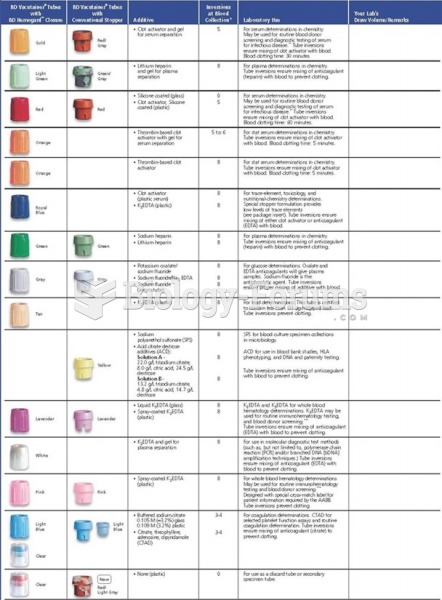 Tube colors, additives, inversions, and laboratory uses.
Tube colors, additives, inversions, and laboratory uses.
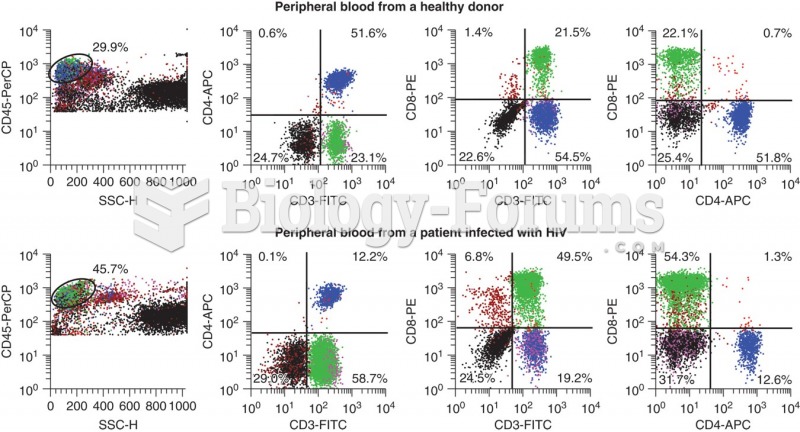 Flow scattergrams showing results on the top set from a healthy donor and on the bottom set from a ...
Flow scattergrams showing results on the top set from a healthy donor and on the bottom set from a ...
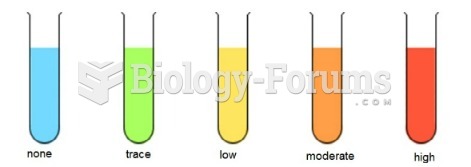 Benedict's test results
Benedict's test results
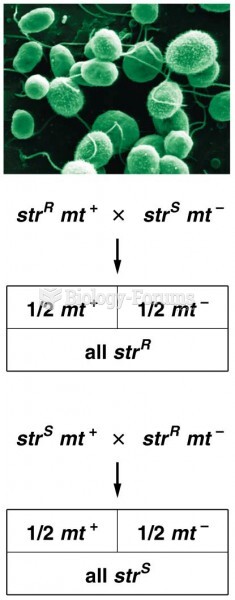 The results of reciprocal crosses between streptomycin-resistant and streptomycin-sensitive
The results of reciprocal crosses between streptomycin-resistant and streptomycin-sensitive