Code the following cases for inpatient facility purposes using ICD-9-CM and ICD-10-CM and PCS codes.
Calculate the MS-DRG.
Identify the principal vs. secondary diagnoses and procedures.
Use external cause codes when appropriate.
Do NOT code procedures that are captured by the facility chargemaster.
Secondary diagnoses and procedures do not need to be sequenced in any particular order.
Enter "None" when no code is required.
INPATIENT HOSPITAL
Health Record Face Sheet
Record Number: 78-50-77
Age: 66
Gender: Female
Length of Stay: 8 Days
Service Type: Inpatient
Discharge Status: To Home
Diagnosis/Procedure: Chest Pain
Congestive Heart Failure
DISCHARGE SUMMARY
PATIENT: MARGARET INPATIENT
RECORD NUMBER: 78-50-77
ADMITTED: 11-26-XX
DISCHARGED: 12-03-XX
PHYSICIAN: DR. ALEX, M.D.
DISCHARGE DIAGNOSES
1. Chest pain, uncertain etiology, myocardial infarction was excluded (based on normal ECG, and normal LDH isoezymes obtained that were 2 days prior to admission). Consider gallbladder abnormality.
2. Elevated liver function tests, which gradually fell through the hospitalization.
3. Dyspnea with organic heart disease as noted above on the echocardiogram. I suspect that much of her dyspnea and congestive heart failure is due to diastolic noncompliance of the left ventricle, and feel that she should be on a calcium blocker to help this.
4. Slow atrial fibrillation: I do not believe that she requires a pacemaker at this time. However, she is not a candidate for any kind of rate slowing drugs. (Procardia is utilized.)
5. She did not receive any diuretics at all through this hospitalization, and maintained stable weight and good urine output.
6. Renal insufficiency: Her renal function improved quite a bit during the admission. It was felt that her renal insufficiency is probably due to a combination of diuretics, Captopril and Voltaren. All of these were discontinued and she did well.
7. Abnormal gallbladder with elevated liver function tests: This requires further follow up as an outpatient.
DISCHARGE MEDICATION:
1. Enteric aspirin 5 grains 1 q. day.
2. Procardia XL, 30 mg 1 q. day.
3. Pepcid 20 mg, 1 q. day.
She is not to take any Bumex, Capoten, Cytotec, or Voltaren. She is to have a double dose oral cholecystogram 1 week from today.
HISTORY: The patient is a 66-year-old female received here in transfer from critical access hospital following chest pain with subsequent renal insufficiency.
LABORATORY DATA: The labs were obtained the day of admission at Harms Memorial Hospital. BUN 70, creatinine 1.6, glucose 136, uric acid 9.2, total bilirubin 0.4, alkaline phosphatase 214, SGPT 108, SGOT 28, LDH 158, GGTP 292, sodium 144, potassium 4.7, cholesterol 300, triglycerides 403. Daily CMP's were obtained.
On second day of hospitalization, lab pertinent values showed BUN 60, Creatinine 1.3, Alk. Phos. 187, SGPT 83, GGTP 256.
Third day of hospitalization labs were BUN 57, creatinine 1.2, alk. phos. 191, SGPT 75, GGTP 252, and on fourth hospitalization day, Glucose 134, Bun 47, creatinine 1.1, uric acid 75, alk. phos 180, SGPT 62, SGOT 25, LDH 139, GGTP 236, albumin 3.7, sodium 144, potassium 4.4, cholesterol 295, triglycerides 285.
ELECTROCARDIOGRAM: Slow atrial fibrillation. Otherwise, this is unchanged.
RADIOLOGIC STUDIES: Gallbladder ultrasound that showed echodensity within the gallbladder consistent with a polyp, slow flowing sludge, or even an adenoma or carcinoma. The wall thickness was normal and there was no dilatation of the intrahepatic biliary tree. The common duct is a little enlarged at 6.5 mm. There appeared to be no stones. An oral cholecystogram is recommended in follow up. A double dose oral cholecystogram was performed and was non-visualizing. Chest x-ray showed cardiomegaly with a globular configuration and pulmonary venous distention consistent with congestive heart failure. Ventilation perfusion lung scan was normal.
Echocardiogram showed a small vigorous left ventricle with concentric left ventricular hypertrophy. There is moderate bi-atrial enlargement and probable atrial septal defect. The right ventricle is of normal size and systolic performance. There is mild aortic valve sclerosis with no stenosis or insufficiency. There is no pericardial effusion.
HOSPITAL COURSE: The patient is admitted to the hospital and multiple tests are obtained. She is initially treated only with oxygen, Pepcid, and aspirin. Procardia XL 30 mg daily was initiated on day one of hospitalization. As noted above, her renal function continued to improve on a daily basis. Her blood sugars were also followed and remained between 115 and 157 throughout the hospitalization on Accu-Cheks. Her blood pressure during the first part of the hospitalization ranged around 100 to 135/70. Toward the latter part of the hospitalization it slowly rose. On the day of discharge, it was 150/80 with a pulse of 50 and respiration of 18, afebrile. Her cardiac telemetry showed slow atrial fibrillation with rate in the high 40s and low 50s for the most part. During the night she does slow somewhat and has pauses, but these are only when she is asleep, and are asymptomatic. They are not excessive. The patient had no chest pain or dyspnea, and felt well.
DISPOSITION: She is to have a double dose oral cholecystogram after discharge from the hospital.
DR. ALEX, M.D.
Electronically authenticated by Dr. Alex, on 12-05-xx, 4434
HISTORY AND PHYSICAL
PATIENT: MARGARET INPATIENT
RECORD NUMBER: 78-50-77
ADMITTED: 11-26-XX
DISCHARGED: 12-03-XX
PHYSICIAN: DR. ALEX, M.D.
CHIEF COMPLAINT: Chest pain.
HISTORY OF PRESENT ILLNESS: The patient is a 66-year-old female received in transfer today from a critical care hospital for evaluation of recent episode of chest pain with subsequently no insufficiency.
The patient has a long history of suspected heart disease. She reports having had MI's 24 years ago and 12 years ago. These are nondocumented. She has a 20-some year history of substernal dull chest pain, relieved in part with nitroglycerin or isordil. It also comes on with exertion, at rest, and occasionally at night. This was increasing quite a bit about 5 years ago. She was tried on calcium blockers and seemed to have some benefit accrued from those. Echocardiogram showed bi-atrial enlargement with concentric LVH, good LV function, and possible ASD. Because of these findings, she had a right and left heart catheterization done five months ago. Oximetry series in the right heart was grossly normal. The green dye curve showed no evidence for a left to right shunt. Pulmonary artery pressure 50/20, mean 32. Right atrial pressure 11, pulmonary wedge pressure is 22 with a 16-18 mm V-wave. The left ventricular and diastolic pressure is 18. Left ventriculogram is normal. There are no aortic or mitral valve gradients. Selective coronary artery angiography is essentially normal with a few minimal irregularities, less than 25%. These are seen in the right coronary artery. The patient since then has really done fairly well until 2 days ago while driving, she had the abrupt onset of dyspnea, flushing a hot feeling, marked diaphoresis, and near syncope. This was associated with moderately severe left sub mammary, hard chest pain that was somewhat pleuritic. She says it is the first time she has ever had a pain like this. Altogether, it lasted about 60 minutes. She has not had any since then. Up until then, she has been feeling fairly well recently. She has not been having much chest pain or dyspnea. She, however, on 11-18 had to increase her pillows at night on her bed from one to two pillows because of orthopnea. She has had no edema, paroxysmal nocturnal dyspnea, or change in her exertional dyspnea. She has no palpitations, light-headed spells, near syncope, or syncope.
DRUG ALLERGIES: She is allergic to Penicillin, Sulfa, Methylate, and Tylenol.
MEDICATIONS: Bumex 0.5 mg, two tablets q. day, Capoten 12.5 mg ½ tablet tid, Quinine one tablet prn for leg cramps, Darvon prn, Voltaren 75 mg bid (sometimes she takes it tid), Cytotec one tablet bid-. Previously she had been on Pepcid, but has not been taking any recently at home. She denies having remembered taking Prilosec.
FAMILY HISTORY: Her mother died of an MI in her 60s.
REVIEW OF SYSTEMS: The patient's past review of systems is remarkable for a long history of atrial fibrillation. She has not smoked in many, many years. She has a 20-year history of hypertension. She has a long history of hyperlipidemia. She has been massively obese in the past and has weighted as much as 300 lbs.
The patient has been a diabetic for a number of years, and has been on insulin off and on since the early 1980s. She has had distant deep venous thrombosis. She has had a venous stripping in her legs in the past. She had a history of gout, manifested as podagra. She has had DJD in the right knee. She has a peripheral sensory neuropathy, but no other complications of her diabetes particularly. She has a history of reactive depression. She has a history of episodic cutaneous candidiasis, and varicose veins and previous history of cystitis. She has nocturnal leg cramps for which she takes Quinine.
The patient was in the hospital 4 months ago with fever, back pain, and Staphylococcal septicemia and septic knee. At that time, she had marked renal insufficiency of acute onset. This seemed to resolve following cutting back on her Capoten and Lasix, as well as with treatment of her septicemia. Her sodium at that time fell to a low of 117. Her BUN rose to a high of 101. Her creatinine rose to 2.4. Her potassium rose to a high of 7.4.
PHYSICAL EXAMINATION: Blood pressure 115/65, pulse 61, respirations 16, afebrile. No jugular venous distention with few bi-basilar rales. Skin is warm and dry. Heart: S1, S2, within normal limits, with a Grade 1/6 systolic ejection murmur at the left upper sternal border. She has minimal, if any, change in a mildly split S2 with respiration. Abdomen is remarkable for mild epigastric tenderness. She is quite obese. There is no peripheral edema.
DIAGNOSTIC STUDIES: ECG is stable, showing slow atrial fibrillation with a rate from about 42 to about 60. PA and lateral chest x-ray shows pulmonary venous distention with Kerley B lines, and cardiomegaly. The configuration is globular. Ventilation-perfusion lung scan done here is basically normal.
LABORATORY DATA: Admission bilirubin 2.5, alk phosphatase 203, amylase 29, SGOT 295, LDH 376. Urinalysis shows 4-6 white cells and 2-4 red cells. Glucose 139, BUN 4.5, creatinine 1.4, chloride 101, CPK 111, LDH 271, sodium 149, potassium 4.6. Subsequent CKs are normal. Blood gas on admission on room air pH 7.42, PC 2 35, PO2 63, bicar 26, saturation 92%. Strep screen is normal. Protime 12.6. Repeat SGOT is 594 with CPK of 75, LDH 727. White count on admission 6,900, Hgb. 12.7, MCV 85, platelets 139,000.
Repeat labs: Glucose 146, BUN 60, creatinine 2.0, total bilirubin 0.7, SGOT 53, LDH 163, CPK 45, cholesterol 281, triglycerides 313, sodium 144, and potassium 5.3.
Repeat labs: Glucose 135, BUN 80, creatinine 2.8, sodium 142, and potassium 6.1. That was at 7:15 a.m. Repeat labs later on in the day: Sodium 141, potassium 5.5, BUN 78, creatinine 2.2, glucose 167, white count 8,500, Hgb. 12.6, platelets 147,000.
LD isoezymes are received. The patient's first three LDHs were 271, 727 and 376. In each case, the ratio of LD1 to LD2 is 0.6. Percent of LD5 rose from 28% on the first, 61% on the second and then fell to 50% on the third. These are all felt to be not reflective of myocardial ischemia, but do show an elevation predominantly due to LD 5.
IMPRESSION:
1. Recent episode of chest pain, dyspnea, and diaphoresis: Myocardial infarction is excluded with normal LD, CKs and serial ECGs. There was a clear rise in LDH predominantly from LD5 isoenzyme, as well as a transient marked rise in SGOT. Admission blood gas is normal and current ventilation-perfusion lung scan is normal. I suspect pulmonary embolism is not particularly likely. Etiology remains unclear.
2. Renal insufficiency: the patient's BUN and creatinine clearly went up (with treatment with Captopril, Bumex and Voltaren) and appeared to be a little better this morning. Will follow patient on this process.
3. Chronic diabetes.
4. Severe hyperlipidemia.
5. Possible ASD on previous echocardiogram, but not substantiated on previous heart catheterization.
6. Elevated filling pressures felt due to diastolic stiffness of the left ventricle, with normal left ventricular systolic performance.
7. Normal coronary arteries in 1986 with borderline elevation of right heart pressures, felt secondary to the elevated wedge.RECOMMENDATIONS: Admit for careful observation and treatment as needed.
DR. ALEX, M.D.
Electronically authenticated by Dr. Alex, on 12-03-xx, 4434
RADIOLOGY REPORT
PATIENT: MARGARET INPATIENT
RECORD NUMBER: 78-50-77
ADMITTED: 11-26-XX
DISCHARGED: 12-03-XX
PHYSICIAN: DR. ALEX, M.D.
CHEST X-RAY
HISTORY: Acute renal failure with shortness of breath.
CHEST:
The heart is enlarged. It appears quite globular in its configuration. Pulmonary venous distension is present with peribronchial thickening and diffuse thickening of the interstitium with Kerley B lines. These findings are all consistent with congestive heart failure. The heart configuration is somewhat globular and may suggest pericardial effusion.
IMPRESSION:
1. Congestive heart failure.
RADIOLOGY REPORT
PATIENT: MARGARET INPATIENT
RECORD NUMBER: 78-50-77
ADMITTED: 11-26-XX
DISCHARGED: 12-03-XX
PHYSICIAN: DR. ALEX, M.D
VENTILATION/PERFUSION LUNG SCAN
HISTORY: Congestive heart failure.
V/P LUNG SCAN:
The patient was administered 11.8 mCi of Xenon-133 gas by inhalation. Single breath, equilibrium and washout images were obtained. The patient was then injected with 3.94 mCi of 99mTc MAA. Orthoganal and both posterior oblique images of the lungs were obtained. The ventilation study shows a diffuse homogeneous distribution of radiopharmaceutical without ventilation defects. No significant air trapping is noted. The perfusion study shows diffuse homogeneous distribution of the radiopharmaceutical throughout all lung fields without segmental or subsegmental defects. There are several areas of increased radiopharmaceutical deposition and these probably represent small clumps of the radiopharmaceutical, which is usually related to MAA preparation and may range from increased amount of aluminum to a poor mixing of the albumin.
IMPRESSION: Basically normal ventilation/perfusion lung scan.
DR. RAY, M.D.
Electronically authenticated by Dr. Ray, 11-28-xx, 34455
ICD-9-CM diagnosis code(s): PDx_____________________
SDx _____________________
ICD-9-CM procedure code(s): PPx_____________________
SPx_____________________
ICD-10-CM diagnosis code(s): PDx_____________________
SDx _____________________
ICD-10-PCS procedure code(s): PPx_____________________
SPx_____________________
MS-DRG: _____________________

 Compare the Final Code with the Documentation
Compare the Final Code with the Documentation
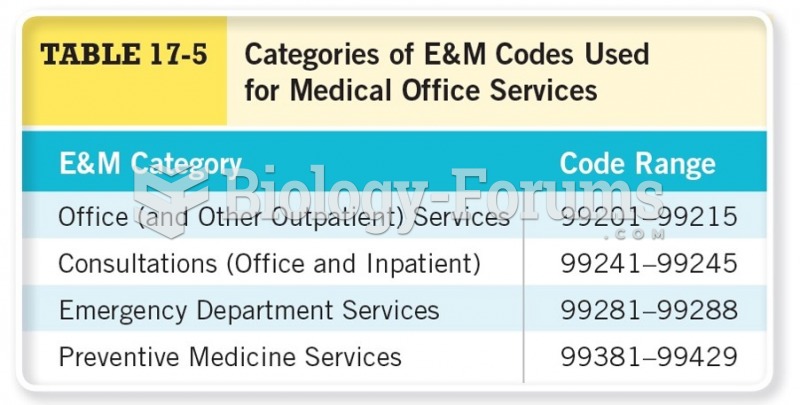 Categories of E&M Codes Used for Medical Office Services
Categories of E&M Codes Used for Medical Office Services
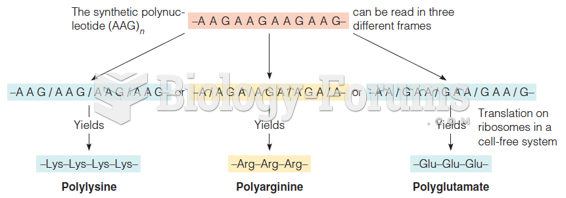 Use of synthetic polynucleotides with repeating sequences to decipher the code
Use of synthetic polynucleotides with repeating sequences to decipher the code
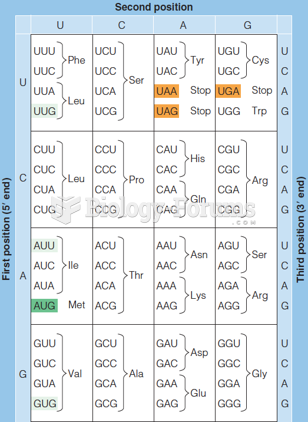 The genetic code (as written in RNA)
The genetic code (as written in RNA)
 Predictions for the results of mutation of an overlapping and a nonoverlapping genetic code
Predictions for the results of mutation of an overlapping and a nonoverlapping genetic code
 Use of synthetic mRNAs to determine genetic code possibilities
Use of synthetic mRNAs to determine genetic code possibilities