Code the following cases for inpatient facility purposes using ICD-9-CM and ICD-10-CM and PCS codes.
Calculate the MS-DRG.
Identify the Principal vs. Secondary diagnoses and procedures.
Use external cause codes when appropriate.
Do NOT code procedures that are captured by the facility chargemaster.
Secondary diagnoses and procedures do NOT need to be sequenced in any particular order. Enter "None" when no code is required.
If more than one occurrence of a procedure is required, report the code with "x 2""x 3" etc.
INPATIENT HOSPITAL
Health Record Face Sheet
Record Number: 73-50-77
Age: 34
Gender: Female
Length of Stay: 2 days
Service Type: Inpatient
Discharge Status: To Home
Diagnosis/Procedure: Repeat cesarean section.
DISCHARGE SUMMARY
PATIENT: LUCINDA INPATIENT
RECORD NUMBER: 73-50-77
ADMITTED: 07-24-XX
DISCHARGED: 07-26-XX
PHYSICIAN: DR. ALEX, M.D.
DIAGNOSIS: Repeat cesarean section at term with single liveborn infant.
HISTORY OF THE PRESENT ILLNESS: This is a 34-year-old Gravida 2, Para 1, female who presents with previous cesarean section, 1 at term for elective repeat cesarean section. The history and physical is unchanged from the office record as updated today.
HOSPITAL COURSE: The patient was taken to the surgical suite where a repeat cesarean section was performed. A viable 8 pound 8 ounce male infant was delivered demonstrating Apgars of 8 at one minute and 9 at five minutes. The baby was taken to the nursery in good condition. The remainder of the hospital course was uneventful with mom and baby recovering nicely. Mom was discharged on day two of hospitalization to home with no complications of surgery and feeling well.
DISCHARGE PLANS: Discharged to home with cesarean wound care instructions. The patient is to return to the office for normal surgical checkup and then at 6 weeks. Instructions to seek help immediately if fever or other complications occur.
DR. ALEX, M.D.
Electronically authenticated by Dr. Alex, M.D., 06-21- xx 8567
HISTORY AND PHYSICAL
PATIENT: LUCINDA INPATIENT
RECORD NUMBER: 73-50-77
ADMITTED: 07-24-XX
DISCHARGED: 07-26-XX
PHYSICIAN: DR. ALEX, M.D.
HISTORY OF PRESENT ILLNESS: This is a 34-year-old Gravida 2, Para 1, female who presents with previous cesarean section x's 1 at term for elective repeat cesarean section. The history and physical is unchanged from the office record as updated on 10-02-xxxx, and a copy of which appears in the chart.
PHYSICAL EXAMINATION:
HEENT/NECK: Examination is clear. The thyroid is normal.
LUNGS: Chest is clear to auscultation.
CARDIOVASCULAR: Heart is regular rate and rhythm with no murmurs.
ABDOMEN: Reveals a 45 cm fundus with good fetal heart tones.
EXTREMITIES: Clear.
GENITORECTAL: Deferred.
IMPRESSION: Previous cesarean section at term.
PLAN: After a thorough discussion earlier in the pregnancy in regard to vaginal birth after cesarean section, its attendant risks and concerns as well as the clinical impression of a small mid pelvis outlet, the patient understands her options and alternatives and I feel freely gives an informed consent for a repeat cesarean section. She presents at this time for this procedure.
DR. ALEX, M.D.
Electronically authenticated by Dr. Alex, M.D., 07-22-xx, 6543
OPERATIVE REPORT
PATIENT: LUCINDA INPATIENT
RECORD NUMBER: 73-50-77
DATE OF SURGERY: 07-24-xx
SURGEON: DR. ALEX, M.D.
ASSISTANT SURGEON: DR. BILLIE, M.D.
PREOPERATIVE DIAGNOSIS: Previous cesarean section at term.
POSTOPERATIVE DIAGNOSIS: Previous cesarean section at term.
OPERATIVE PROCEDURE: Repeat low cervical transverse cesarean section.
COUNTS: Instrument and sponge count were correct.
ESTIMATED BLOOD LOSS: 600 cc.
DESCRIPTION: After a satisfactory level of spinal anesthesia was obtained the patient as prepped and draped in the supine position in the usual manner for abdominal surgery. The abdomen was entered by excision into the old Pfannenstiel scar and a low cervical transverse cesarean section performed. A viable 8 pound 8 ounce male infant was delivered demonstrating Apgars of 8 at 1 minute and 9 at 5 minutes when evaluated by the attending nursing personnel. The placenta and membranes were removed and the endometrium bluntly curetted with the surgeons fingers and covered with a moist lap. The endometrium was then closed with cutaneous 0 Vicryl. The myometrium was imbricated using 0 Vicryl and vertical Limberg suture technique with good hemostasis. The serosa was then closed with continuous 2-0 Vicryl and all free blood and clot removed from the pelvic cavity bilaterally. The anterior peritoneum was closed with cutaneous 2-0 Vicryl. The fascial remnants in the midline were approximated with interrupted 0 Vicryl and the fascia itself was closed with continuous 0 Vicryl using 2 sutures overlapped in the midline. The subcutaneous dead space was closed in multiple layers of 3-0 Vicryl and 4-0 Vicryl subcuticular was used to approximate the skin edges. Steri-Strips and a sterile dressing applied. The procedure was terminated. The patient tolerated this procedure well and was transferred to the recovery room awake and in satisfactory condition.
DR. ALEX, M.D.
Electronically authenticated by Dr. Alex, M.D., 07.25.xx 3211
ICD-9-CM diagnosis code(s): PDx_____________________
SDx _____________________
ICD-9-CM procedure code(s): PPx_____________________
SPx_____________________
ICD-10-CM diagnosis code(s): PDx_____________________
SDx _____________________
ICD-10-PCS procedure code(s): PPx_____________________
SPx_____________________
MS-DRG: _____________________

 ANA code of ethics
ANA code of ethics
 Select the Code with the Highest Level of Specificity
Select the Code with the Highest Level of Specificity
 Corroded terminals on a waste-spark coil can cause misfire diagnostic trouble codes to be set.
Corroded terminals on a waste-spark coil can cause misfire diagnostic trouble codes to be set.
 A plastic MAP sensor used for training purposes showing the electronic circuit board and electrical ...
A plastic MAP sensor used for training purposes showing the electronic circuit board and electrical ...
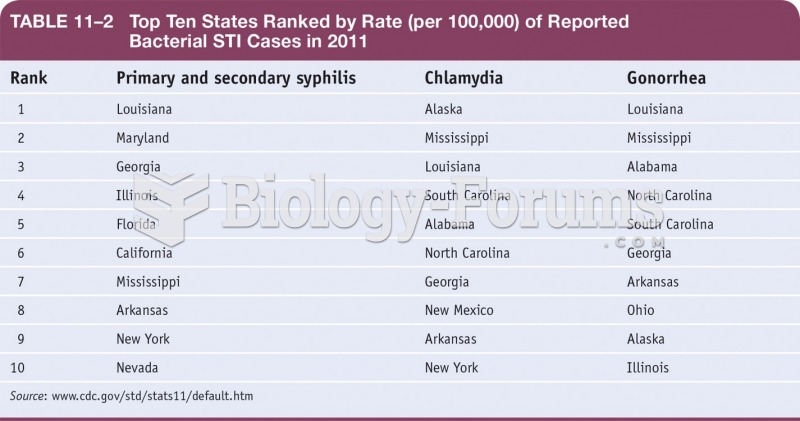 Top Ten States Ranked by Rate or Reported Bacterial STI Cases in 2011
Top Ten States Ranked by Rate or Reported Bacterial STI Cases in 2011
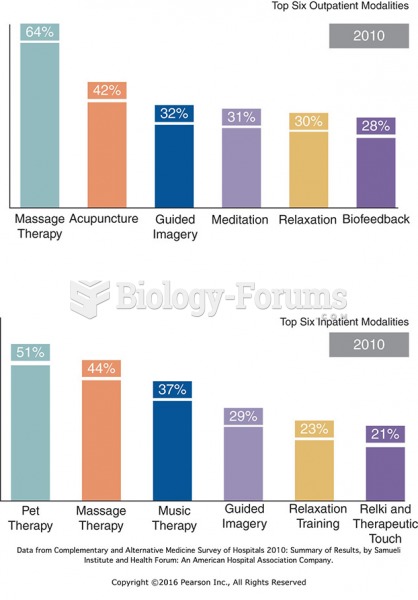 Top Six Hospital Outpatient and Inpatient CAM Therapies.
Top Six Hospital Outpatient and Inpatient CAM Therapies.