Code the following cases for inpatient facility purposes using ICD-9-CM and ICD-10-CM and PCS codes.
Calculate the MS-DRG.
Identify the Principal vs. Secondary diagnoses and procedures.
Use external cause codes when appropriate.
Do NOT code procedures that are captured by the facility chargemaster.
Secondary diagnoses and procedures do NOT need to be sequenced in any particular order. Enter "None" when no code is required.
If more than one occurrence of a procedure is required, report the code with "x 2""x 3" etc.
INPATIENT HOSPITAL
Health Record Face Sheet
Record Number: 81-50-77
Age: 32
Gender: Male
Length of Stay: 2 Days
Service Type: Inpatient
Discharge Status: To Home
Diagnosis/Procedure: Foreign Body Left Ankle
DISCHARGE SUMMARY
PATIENT: PATRICK INPATIENT
RECORD NUMBER: 81-50-77
ADMITTED: 10-15-XX
DISCHARGED: 10-17-XX
PHYSICIAN: DR. ALEX, M.D.
DISCHARGE DIAGNOSIS: Healing fracture left ankle with retained foreign body implant.
PROCEDURE(S): Removal of foreign body implant from left ankle (K-wire and screw).
HISTORY OF THE PRESENT ILLNESS: This 32-year-old male patient is admitted for removal of hardware from his left ankle. History reveals that the patient sustained a fracture of his left ankle 4 years ago. The patient sustained the ankle fracture after jumping off a train while working in the rail yard and turned his ankle. The patient has been symptom free until recently when started having some pain and problems with his ankle. He presents now requesting to have the hardware removed from the healed ankle.
LABORATORY DATA: We obtained blood for CBC, Chem screen, PT, PTT and a urinalysis. We did an EKG, which shows a normal sinus rhythm. There-are no acute ST or T-wave changes and a chest x-ray was also done which is not particularly remarkable, other than borderline cardiomegaly
HOSPITAL COURSE: The patient underwent removal of hardware with no complications and was discharged on the morning of day 2.
DISCHARGE PLANS: The patient was discharged with prescription for pain medication as needed and to return for post op checkup as scheduled or call to be seen immediately for any sign of infection or complication.
DR. ALEX, M.D.
Electronically authenticated by Dr. Alex, M.D., 10-21-xx 4887
HISTORY AND PHYSICAL
PATIENT: PATRICK INPATIENT
RECORD NUMBER: 81-50-77
ADMITTED: 10-15-XX
DISCHARGED: 10-17-XX
PHYSICIAN: DR. ALEX, M.D.
CHIEF COMPLAINT: Foreign body of the left ankle.
HISTORY OF PRESENT ILLNESS:
This 32-year-old male patient is admitted for removal of hardware from his left ankle. History reveals that the patient sustained a fracture of his left ankle 4 years ago. The patient sustained the ankle fracture after jumping off a train while working in the rail yard and turned his ankle. The patient has been symptom free until recently when started having some pain and problems with his ankle. He presents now requesting to have the hardware removed from the healed ankle. He is admitted to the hospital now for surgery.
DRUG ALLERGIES: No known drug allergies.
MEDICATIONS: None.
SURGERIES: History of open reduction and internal fixation of the left ankle 4 years ago.
MEDICAL ILLNESS: Patient is a healthy appearing male with no known medical illnesses at this time.
REVIEW OF SYSTEMS:
HEENT: No history of headaches, blurred vision, double vision or loss of vision. No history of frequent sore throats, nose bleeds or neck pain.
CHEST: No shortness of breath, diaphoresis, palpitation or chest pain.
ABDOMEN: No history of nausea, vomiting, diarrhea or weight loss.
GU: No history of dysuria, frequency, hesitancy, urgency or hematuria.
PHYSICAL EXAM:
GENERAL: Alert and cooperative male who appeared to be in no acute distress.
HEENT: Head was normocephalic. Pupils are equal and react to light and accommodation. Extraocular muscles are intact. Oropharynx and nasopharynx are within normal limits.
NECK: Supple. No evidence of any lymphadenopathy.
CHEST: Clear.
HEART: Regular rate and rhythm. No murmurs.
ABDOMEN: Soft, no masses.
GU: That of a normal male.
ADMITTING DIAGNOSIS: Healed left ankle fracture with retained foreign body.
PLAN: The patient will be admitted to the hospital for removal of hardware from his left ankle. Procedure, sequelae, alternatives and complications were discussed and the patient wishes to proceed.
DR. ALEX, M.D.
Electronically authenticated by Dr. Alex, M.D., 10-15-xx 4887
OPERATIVE REPORT
PATIENT: PATRICK INPATIENT
RECORD NUMBER: 81-50-77
SURGERY DATE: 10-15-XX
SURGEON: DR. ALEX, M.D.
PREOPERATIVE DIAGNOSIS: Healing fracture left ankle with retained foreign body implant.
POSTOPERATIVE DIAGNOSIS: Healing fracture left ankle with retained foreign body implant.
OPERATIVE PROCEDURE: Removal of foreign body implant from left ankle (K-wire and screw).
ANESTHESIA: General
DESCRIPTION: The patient was taken to the operating room and placed on the operating table in a supine position. after he was adequately anesthetized using general inhalation anesthesia , tourniquet was placed high on the groin of the left leg, which was elevated and prepped with Betadine and properly placed sterile drapes. Small incision was made over the medial malleolus at the site of the previous incision. It was carried down through the subcutaneous tissues. Using fluoroscopy, the K-wire and the screw were identified, the deltoid ligament was sharply split, and the K-wire and the screw were removed. The split in the deltoid was then repaired using 2-0 Vicryl simple interrupted sutures. The skin was dosed using 3-0 Ethilon vertical mattress sutures. Sterile dressing was placed on the patient and the patient returned to the recovery room in satisfactory condition.
DR. ALEX, M.D.
Electronically authenticated by Dr. Alex, M.D., 10-15-xx 4887
RADIOLOGY REPORT
PATIENT: PATRICK INPATIENT
RECORD NUMBER: 81-50-77
DATE: 10-15-XX
PHYSICIAN: DR. ALEX, M.D.LEFT ANKLE
HISTORY: Healed left ankle fracture status post hardware removal.
LEFT ANKLE:
Two images have been exposed with the C-arm demonstrating no residual screws or pins in the medial malleolus. Calcifications are present between the distal tibia and fibula from previous damage to the interosseous ligaments. The medial malleolar fracture has healed in anatomical alignment.
DR. RAY, M.D.
Electronically authenticated by Dr. Ray, M.D., 10-15-xx 2254
ICD-9-CM diagnosis code(s): PDx_____________________
SDx _____________________
ICD-9-CM procedure code(s): PPx_____________________
SPx_____________________
ICD-10-CM diagnosis code(s): PDx_____________________
SDx _____________________
ICD-10-PCS procedure code(s): PPx____________________
SPx_____________________
MS-DRG: _____________________

 These older adults are participating in an exercise class at their assisted-living facility
These older adults are participating in an exercise class at their assisted-living facility
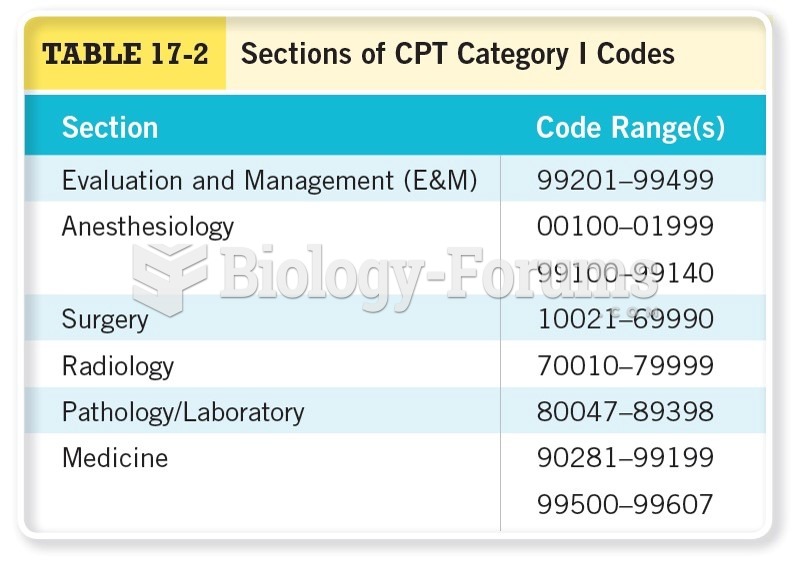 Sections of CPT Category I Codes
Sections of CPT Category I Codes
 Example of standalone and indented codes.
Example of standalone and indented codes.
 The battery was replaced in this Acura and the radio displayed “code” when the replacement ...
The battery was replaced in this Acura and the radio displayed “code” when the replacement ...
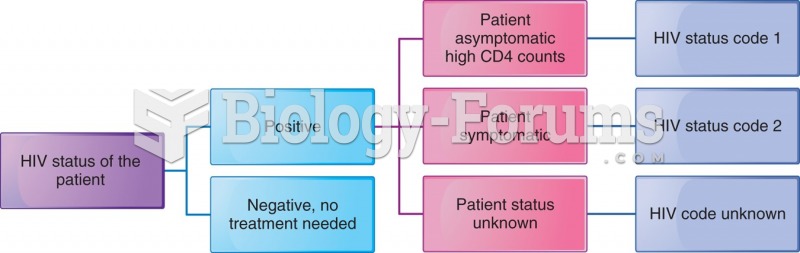 Risk assessment codes for an HIV-infected patient.
Risk assessment codes for an HIV-infected patient.
 Predictions for the results of mutation of an overlapping and a nonoverlapping genetic code
Predictions for the results of mutation of an overlapping and a nonoverlapping genetic code