This topic contains a solution. Click here to go to the answer
|
|
|

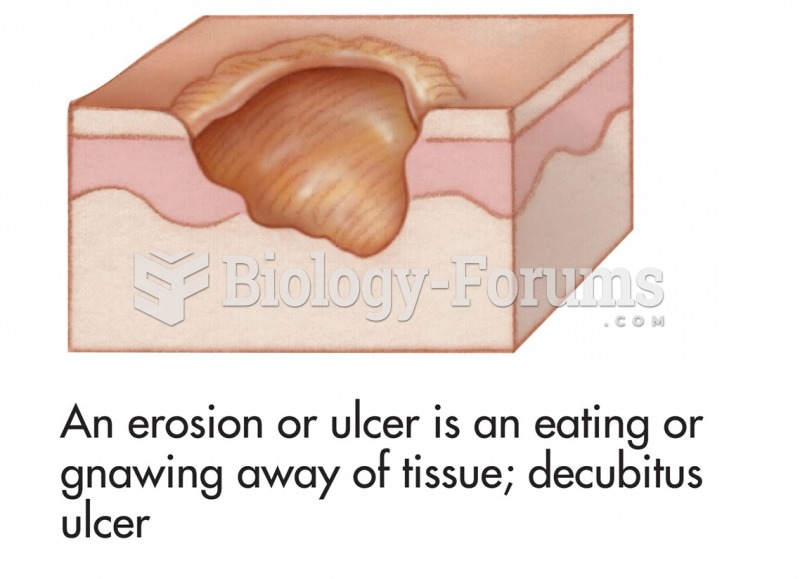 Common skin signs are often evidence of an illness or disorder. An erosion or ulcer is an eating or ...
Common skin signs are often evidence of an illness or disorder. An erosion or ulcer is an eating or ...
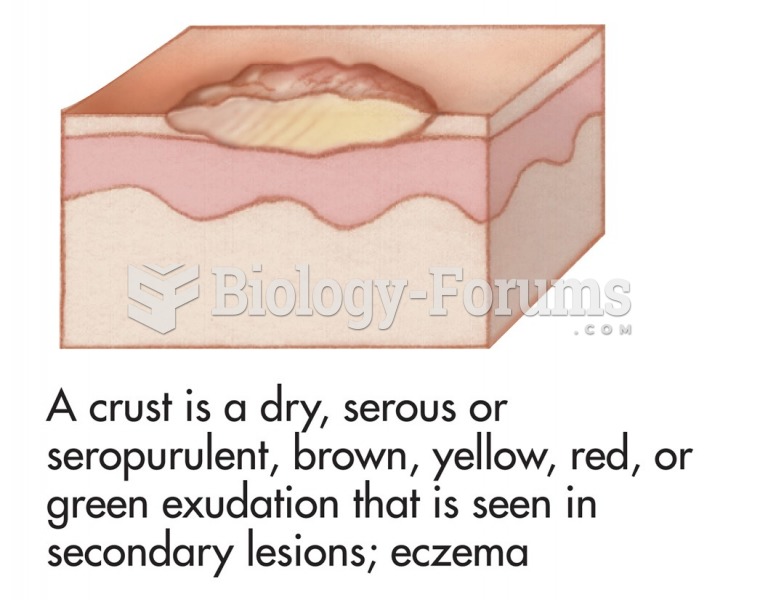 Common skin signs are often evidence of an illness or disorder. A crust is a dry, serous or ...
Common skin signs are often evidence of an illness or disorder. A crust is a dry, serous or ...
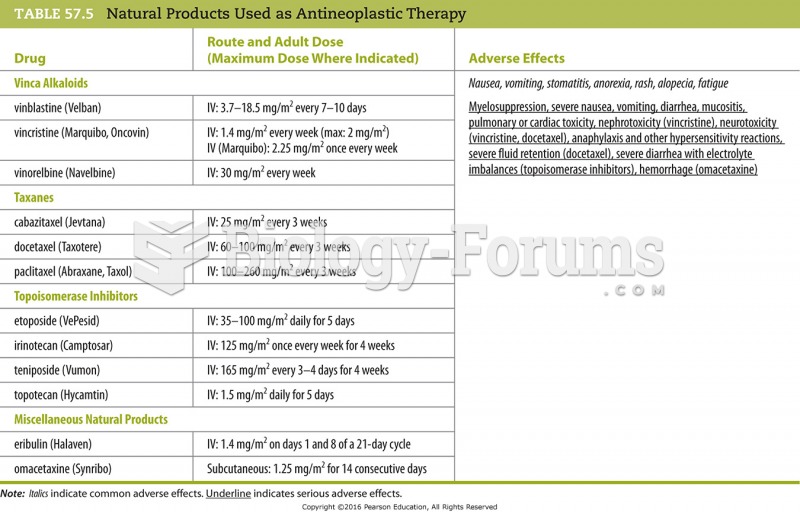 Natural Products Used as Antineoplastic Therapy
Natural Products Used as Antineoplastic Therapy
 A Bear Automotive starting and charging tester. This tester automatically loads the battery for 15 ...
A Bear Automotive starting and charging tester. This tester automatically loads the battery for 15 ...
 The Wisconsin Card Sorting Test. This woman is just starting the test. If she places the first card ...
The Wisconsin Card Sorting Test. This woman is just starting the test. If she places the first card ...
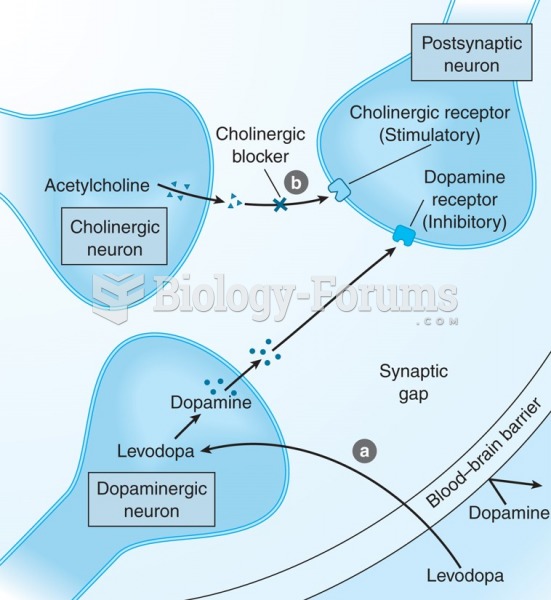 Mechanism of action of anti-parkinson drugs. (a) Levodopa therapy increases dopamine production; (b) ...
Mechanism of action of anti-parkinson drugs. (a) Levodopa therapy increases dopamine production; (b) ...