Answer to Question 1
ANS: B
Protein C has a 6-hour half-life, and so it rapidly decreases when warfarin therapy is begun, along with factor VII (both are vitamin Kdependent proteins). Full anticoagulation with warfarin is not obtained until factors X and prothrombin are decreased to less than 50, requANS: B
Protein C has a 6-hour half-life, and so it rapidly decreases when warfarin therapy is begun, along with factor VII (both are vitamin Kdependent proteins). Full anticoagulation with warfarin is not obtained until factors X and prothrombin are decreased to less than 50, requiring 4 to 7 days based on their half-lives. Because protein C is important in controlling clot formation, its decrease actually puts the patient in a prethrombotic state until full anticoagulation is obtained.
iring 4 to 7 days based on their half-lives. Because protein C is important in controlling clot formation, its decrease actually puts the patient in a prethrombotic state until full anticoagulation is obtained.
Answer to Question 2
ANS: D
The clinical laboratory scientist must immediately call the healthcare provider because this is a critical INR result and he or she must be able to intervene with appropriate patient care. The call must be documented according to the protocol established by clinical scientists in the laboratory. This is essential to prevent a bad outcome for the patient.

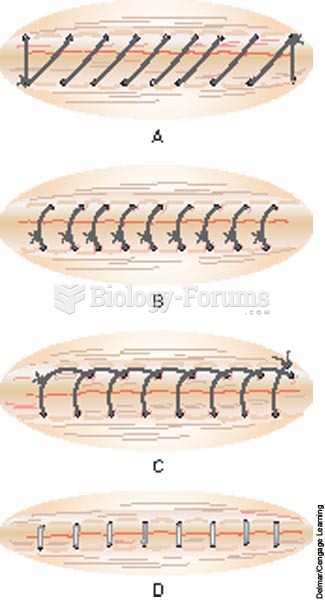 Skin closure methods
Skin closure methods
 A group therapy session.
A group therapy session.
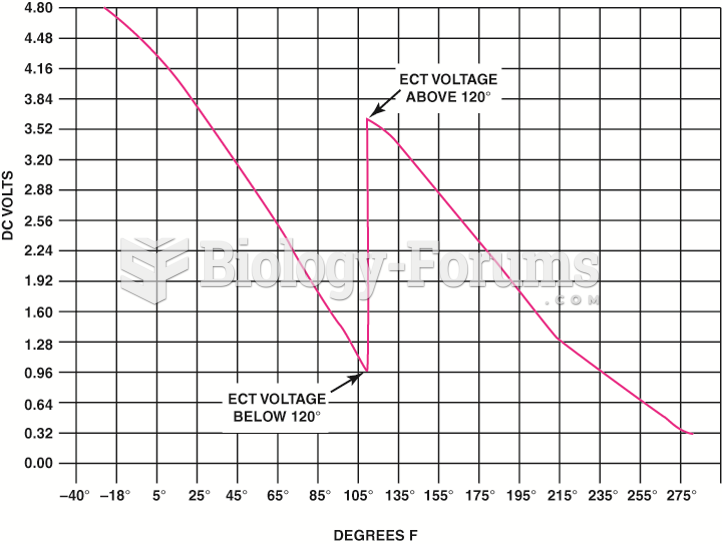 The transition between steps usually occurs at a temperature that would not interfere with cold ...
The transition between steps usually occurs at a temperature that would not interfere with cold ...
 Hands-on class in a massage therapy program.
Hands-on class in a massage therapy program.
 Proteins play an important role in keeping your skin healthy and your nails strong
Proteins play an important role in keeping your skin healthy and your nails strong
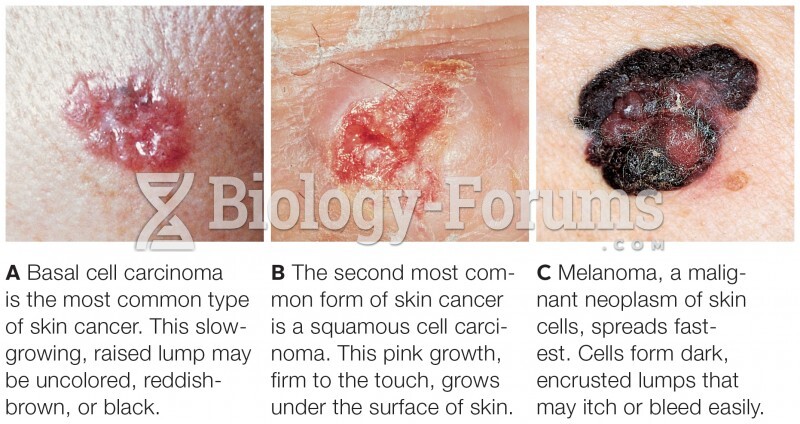 Skin Cancers
Skin Cancers