Answer to Question 1
The American College of Gastroenterology (ACG) uses the Rome III criteria to diagnose IBS. The basis for these criteria, according to the ACG, is that IBS experts have met in Rome for the past 15 years to decide what methods are best used to diagnose IBS.
Rome III as diagnostic criteria are accurate about 65-100 of the time, according to the ACG.
The Rome III criteria include:
Recurrent abdominal pain or discomfort at least 3 months in the last year with two or more of the following:
Improvement of pain with defecation
Onset associated with change in frequency of stool
Onset associated with change in appearance of stool
Physician has ruled out other inflammatory and GI disorders with similar symptoms
Other symptoms may include:
Altered bowel habits or motility (key symptom)
Diarrhea
Constipation
Mixedpt. experiences both constipation and diarrhea
Lower abdominal pain (key symptom)
Flatulence
Gas
Upper GI symptoms including:
Reflux
Chest pain (non-cardiac)
The physician was able to diagnose Ms. Clarke with IBS because:
- She experiences both bouts of constipation and diarrhea for many years
- She complains of several accidents, being unable to make it to the restroom on time
- She endures daily abdominal pain
- Lately several episodes of diarrhea daily (may be evident due to dry mucous membranes - dehydration)
- Hyperactive bowel sounds
Answer to Question 2
Since feeding a critically ill surgical patient is a high priority for proper recovery and healing, there is a decision-making process that occurs to determine the route for nutrition support. For any patient, PO intake is the preferred choice in order to meet nutritional needs as naturally as possible. However, for critically ill patients such as Mr. Perez, this is not possible because he is mechanically ventilated and recent surgeries to the GI tract. According to the ASPEN guidelines, enteral nutrition would be appropriate for this patient if the GI tract is at least partially functional, there is no intestinal hemorrhage, no ileus or fistulas are present, no intractable vomiting is present, and no short bowel syndrome is present. Unfortunately, for this patient, some of these requirements for EN are not met, such as intestinal hemorrhage and the recent surgeries to the GI tract (removal of proximal jejunum resulting in discontinuity and followed by an anastomotic leak) that interrupts GI function. Due to these contraindications and the inability to meet at least 60 of his nutritional needs by EN, TPN was started for this patient. Additionally, since Mr. Perez is critically ill, nutritional support should be provided within the first 24-48 hours from admission.
This patient was S/P a traumatic event and in metabolic stress, meaning it was imperative to begin nutrition support as soon as feasibly possibly, optimally within 24-48 hours after admission into the ICU. Additionally, small amounts of EN (trophic feeds) were started along with PN in order to maintain gut integrity and intestinal mucosa; however, there is a potential for gut ischemia and necrosis if more than trophic EN was administered to meet all of this patient's nutritional needs. Due to the positive outcomes of open abdomen healing and EN (earlier closure rate, reduced fistula formation, and reduced mortality), it is important to wean this patient from TPN and have EN provide the majority of Mr. Perez's nutrition

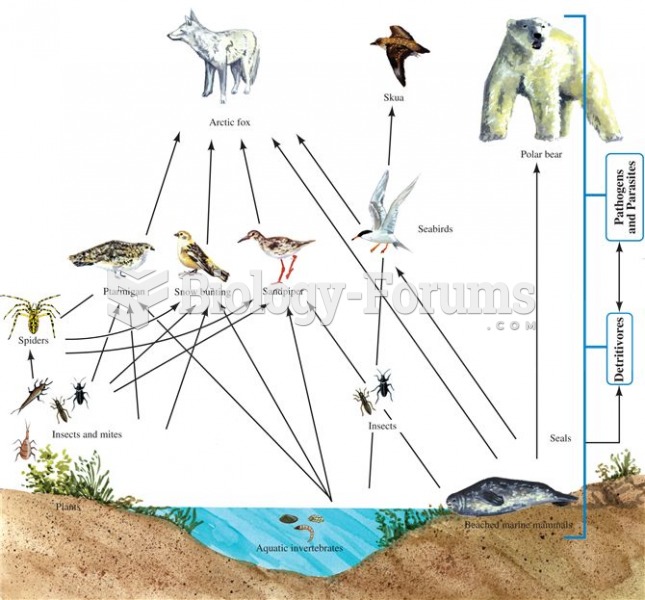 Simple food web of an Arctic island. NOTE: The indication of detritivores and pathogens was not part
Simple food web of an Arctic island. NOTE: The indication of detritivores and pathogens was not part
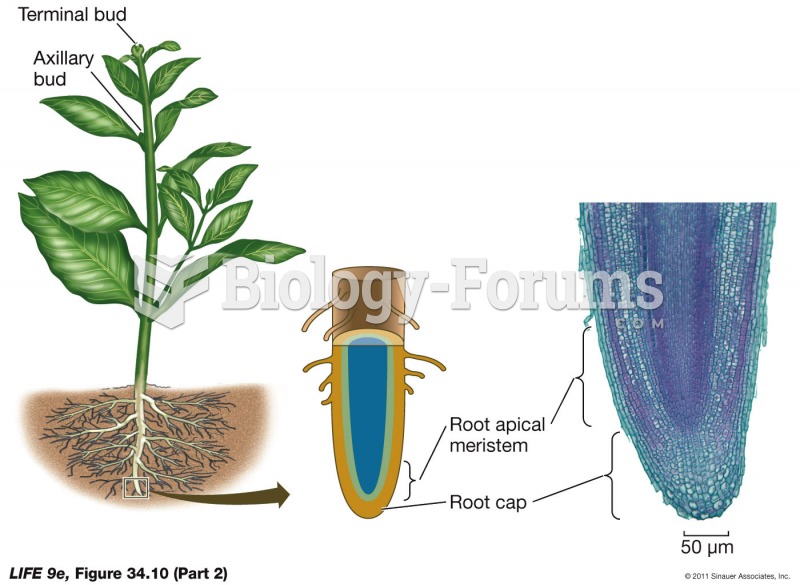 Apical and Lateral Meristems (Part 2)
Apical and Lateral Meristems (Part 2)
 Faith Ringgold, Tar Beach, Part I of the series Woman on a Bridge.
Faith Ringgold, Tar Beach, Part I of the series Woman on a Bridge.
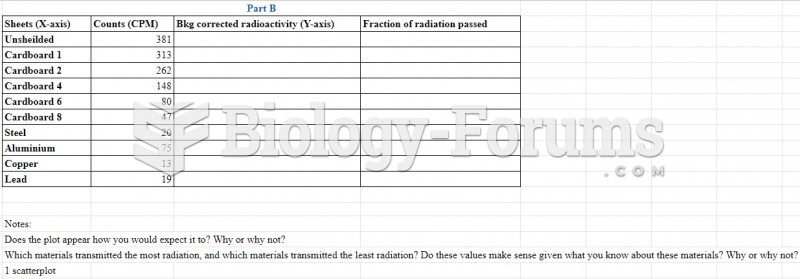 part b
part b
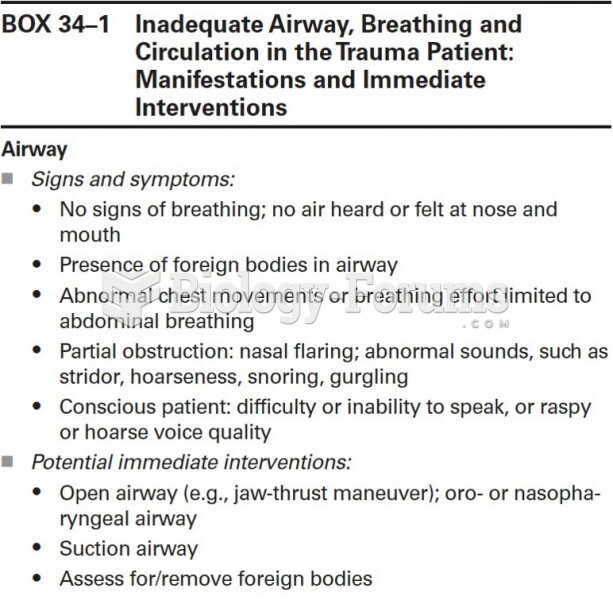 Inadequate Airway, Breathing and Circulation in the Trauma Patient (Part 1)
Inadequate Airway, Breathing and Circulation in the Trauma Patient (Part 1)
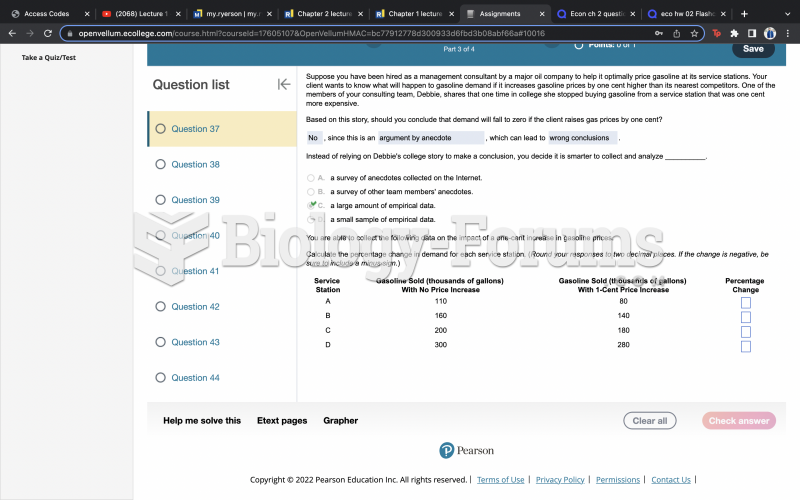 Question 37 Part 2
Question 37 Part 2