Answer to Question 1
Major nutrient and metabolic changes that can occur during an AKI include a rapid decrease in urine output, which can lead to acidosis, electrolyte imbalances (hyperkalemia, hyperphosphatemia), fluid disturbances, impaired glucose utilization, protein catabolism, and accumulation of metabolic waste products.
Energy: 25-35 kcal/kg based on the stress and normal nutrition status of the patient before the injury (if the patient was malnourished beforehand, he would have higher energy needs than this)
Impaired glucose utilization and protein catabolism from uremia
Protein needs range from 0.8 to 2.0 g/kg/d
non-catabolic, not dialyzed: 0.8-1.0 g/kg/d
on renal replacement therapy: 1.0-1.5 g/kg/d
hypercatabolic, receiving CRRT: up to 2.0 g/kg/d
Hyperglycemia may arise due to calories from CRRT and response to metabolic stress
Insulin may be needed due to insulin resistance resulting from AKI
Serum TG should be within normal range if started on enteral or parenteral nutrition because a high TG value may indicate a reduced hepatic capacity for removal of long-chain and medium-chain fatty acids; if TG are high at first, these levels will need to be monitored closely for tolerance.
Answer to Question 2
Lifestyle modifications
- Wt reduction
- DASH eating plan
- Physical activity
- Moderation of alcohol consumption
Pharmacologic
- ACEIs (angiotensin-converting enzyme inhibitors)
- ARBs (angiotensin receptor blockers)
- BBs (beta blockers)
- CCBs (calcium channel blockers)
- Thiazide-type diuretics
Smoking cessation
Wt. loss

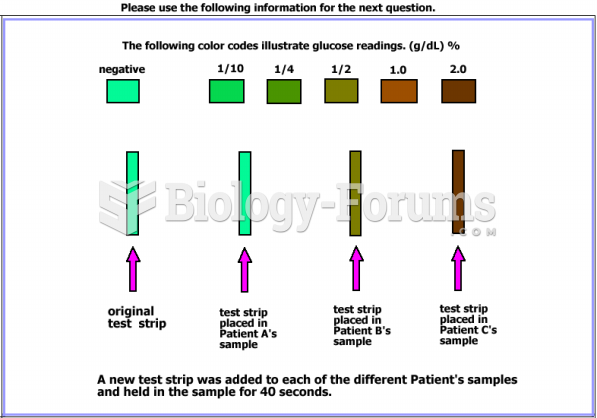 Are the resutls from the glucose strip test consistent with the results obtained from the ...
Are the resutls from the glucose strip test consistent with the results obtained from the ...
 Casting numbers on major components can be either cast or stamped.
Casting numbers on major components can be either cast or stamped.
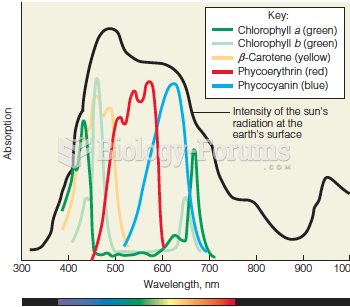 Absorption spectra and light energy
Absorption spectra and light energy
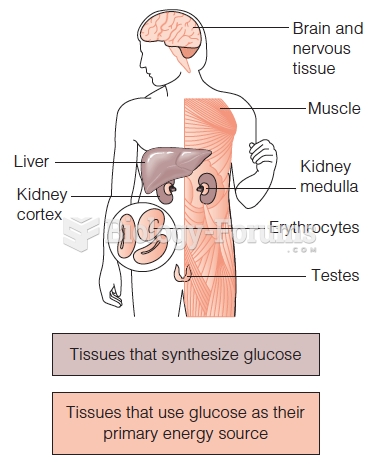 Synthesis and use of glucose in the human body
Synthesis and use of glucose in the human body
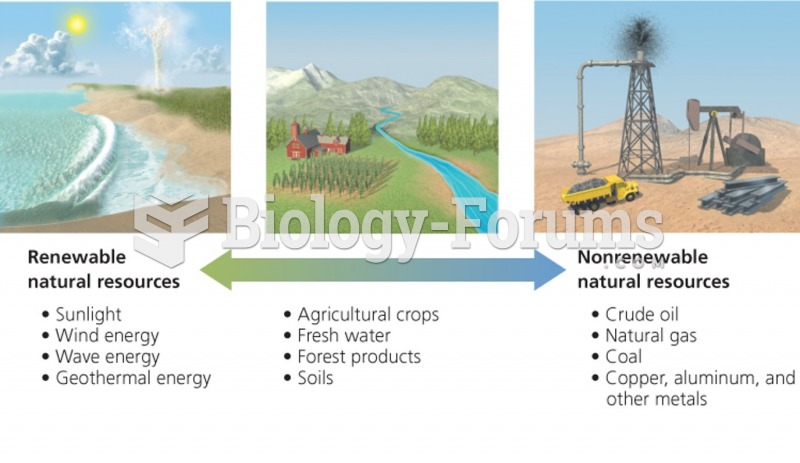 Energy Resources range from inexhaustible to nonrenewable
Energy Resources range from inexhaustible to nonrenewable
 Antibiotic Inhibitors of Protein Synthesis
Antibiotic Inhibitors of Protein Synthesis