This topic contains a solution. Click here to go to the answer
|
|
|

 The grey nurse shark is critically endangered on the Australian east coast.
The grey nurse shark is critically endangered on the Australian east coast.
 The nurse applies a pulse oximeter sensor on the client’s finger.
The nurse applies a pulse oximeter sensor on the client’s finger.
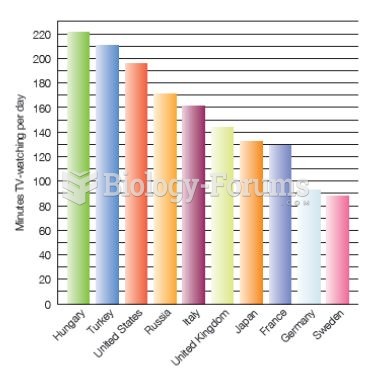 International Television Viewing Rates in Childhood In most developed countries, children watch TV
International Television Viewing Rates in Childhood In most developed countries, children watch TV
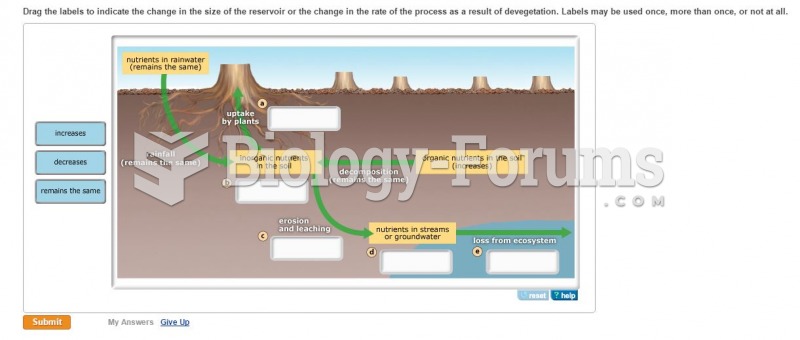 Drag the labels to indicate the change in the size of the reservoir. . .
Drag the labels to indicate the change in the size of the reservoir. . .
 Effleurage to transition to forearm-distal to proximal. Apply effleurage with moderate pressure to ...
Effleurage to transition to forearm-distal to proximal. Apply effleurage with moderate pressure to ...
 How to solve an exponential growth problem involving bacterial growth (Question 1)
How to solve an exponential growth problem involving bacterial growth (Question 1)