This topic contains a solution. Click here to go to the answer
|
|
|

Did you know?
Methicillin-resistant Staphylococcus aureus or MRSA was discovered in 1961 in the United Kingdom. It if often referred to as a superbug. MRSA infections cause more deaths in the United States every year than AIDS.

 Cottontails' ears have developed to hear even whisper-quiet sounds at incredible distances.
Cottontails' ears have developed to hear even whisper-quiet sounds at incredible distances.
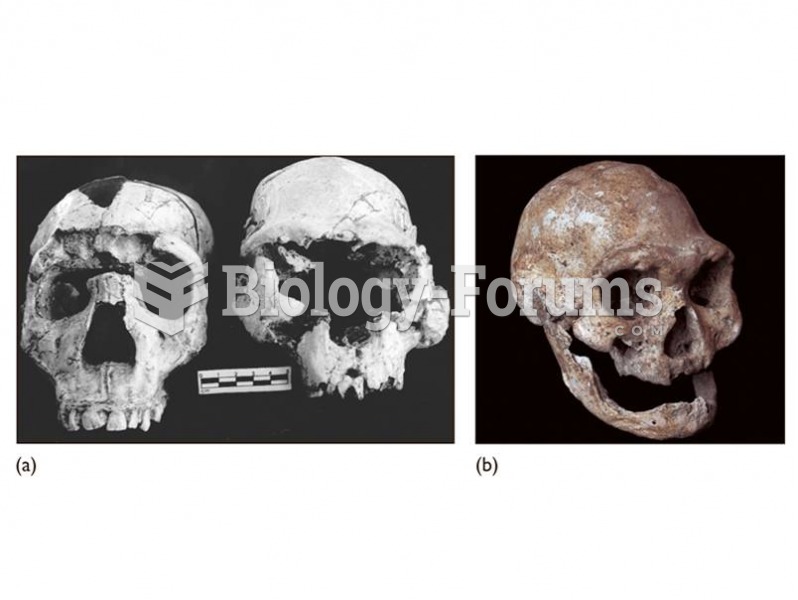 (a) The Dmanisi cranium (right) shows similarities to early African H. erectus including the Narioko
(a) The Dmanisi cranium (right) shows similarities to early African H. erectus including the Narioko
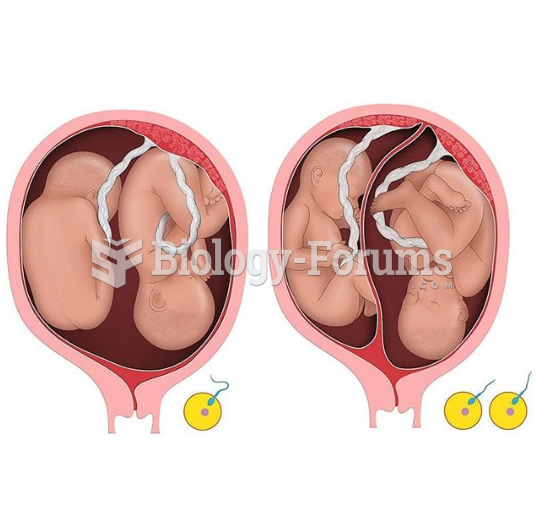 identical (left) and fraternal (right) twins
identical (left) and fraternal (right) twins
 Toys and Gender Labels (1 of 2)
Toys and Gender Labels (1 of 2)
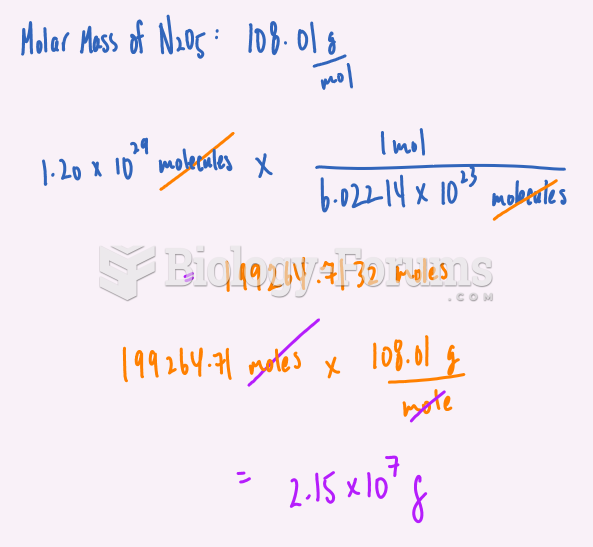 Chemistry Problem Worked Out
Chemistry Problem Worked Out
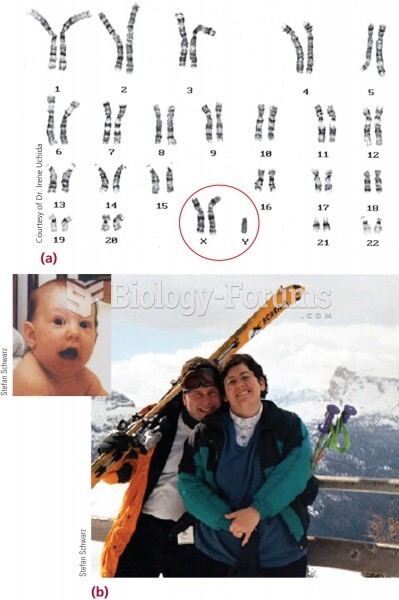 (a) The characteristic karyotype of Klinefelter syndrome. (b) The young man (left) in these photos h
(a) The characteristic karyotype of Klinefelter syndrome. (b) The young man (left) in these photos h