Answer to Question 1
ANS: 2
The R in FOCUS charting is the client's response. In this case, the nurse would document, My arm feels better. Infiltrated IV line would be documented as D referring to data in FOCUS charting. Elevation of left forearm is the A in FOCUS charting. It describes the ac-tion or nursing intervention. Slight hematoma on left forearm is the D referring to data in FOCUS charting.
Answer to Question 2
ANS: 4
Each entry should begin with the time and end with the signature and title of the person record-ing the entry. All entries should be recorded legibly and in black ink because pencil can be erased. The nurse should never erase entries, never use correction fluid, or never use a pencil. The use of correction fluid could make the charting become illegible and it may appear as if the nurse were attempting to hide something or to deface the record. If the physician made an error, the nurse should not document it in the client's chart. It should be documented in an incident report.

 NUrse
NUrse
 A cast of LB1 (left) was compared to several microcephalic skulls, amongst which is that of the micr
A cast of LB1 (left) was compared to several microcephalic skulls, amongst which is that of the micr
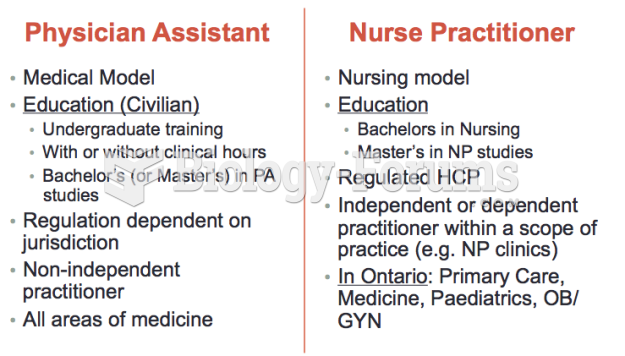 Differences between a Nurse Practitioner
Differences between a Nurse Practitioner
 The client is positioned for the examination
The client is positioned for the examination
 Problem
Problem
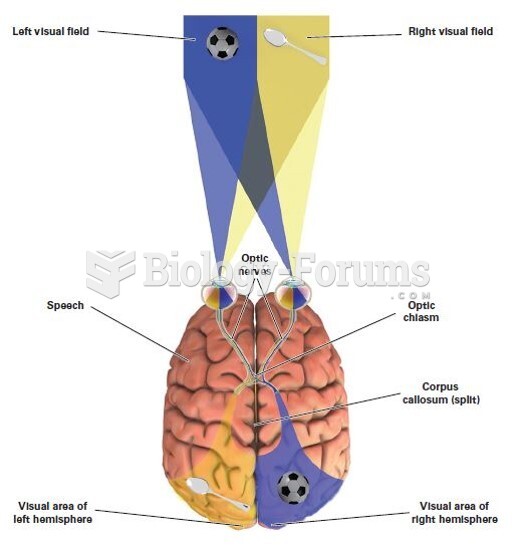 Right and Left Visual Fields
Right and Left Visual Fields